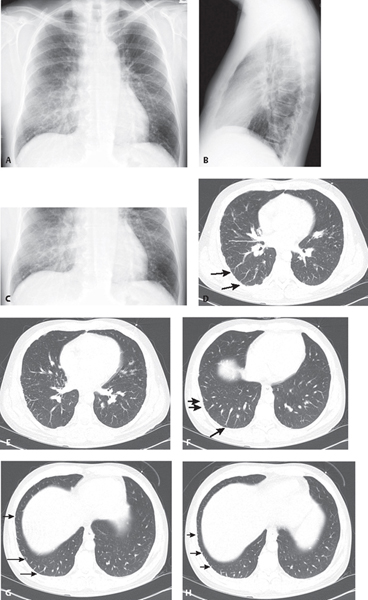
CASE 148 37-year-old man with long-standing history of alcohol abuse and liver disease admitted with an acute episode of gastrointestinal bleeding and progressive dyspnea PA (Fig. 148.1A) and lateral (Fig. 148.1B) chest radiograph with accompanying PA view coned to the lung bases (Fig. 148.1C) demonstrates abnormal peripheral basilar reticular opacities. There is no evidence of heart failure or pleural effusion. Chest CT (lung window) (Figs. 148.1D, 148.1E, 148.1F, 148.1G, 148.1H) shows the reticular opacities representing multiple dilated distal pulmonary arteries that do not taper normally and extend to the pleural surface (long arrows) and juxtapleural telangiectasia (short arrows). Hepatopulmonary Syndrome None Hepatopulmonary syndrome (HPS) is defined by the triad of liver disease, increased alveolar-arterial oxygen gradient ≥15 mm Hg while breathing room air, and intrapulmonary vascular dilatations. HPS develops in 15–20% of patients with cirrhosis. There are two types based on pulmonary angiography. Type I is the most common (86%) and manifests as distal vascular dilatation with juxtapleural telangiectasia. Type II (14%) is characterized by the formation of small, discrete peripheral arteriovenous malformations. It is postulated that HPS is due to increased hepatic production or decreased hepatic clearance of vasodilators, particularly nitric oxide, by the impaired liver. This results in precapillary pulmonary artery dilatation, the formation of direct arteriovenous communications, and dilated pleural vessels. The vascular dilatation causes over-perfusion of the lung relative to its ventilation, leading to ventilation-perfusion mismatch and hypoxemia. HPS manifests clinically as progressive dyspnea, cyanosis, spider nevi, and digital clubbing in a patient with cirrhosis. Patients may also complain of platypnea and have orthodeoxia. Pulmonary artery pressures are usually normal or reduced. Fig. 148.1
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Findings
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine




