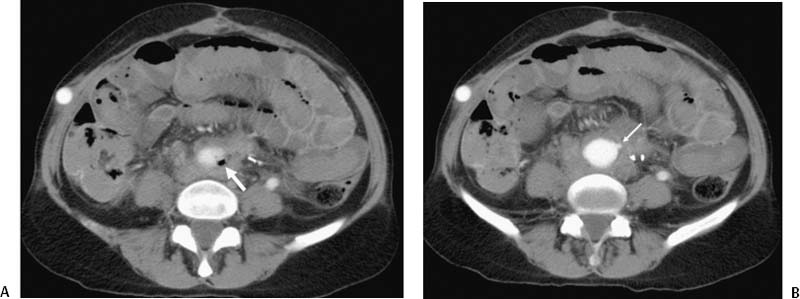
CASE 15 A 68-year-old female presented to the emergency room with bright red blood per rectum. Her history was remarkable for insertion of an aortobi-femoral bypass graft to treat an abdominal aortic aneurysm. This graft later occluded but was left in situ. An axillofemoral and a femoral-to-femoral bypass graft were placed to provide flow to the legs. After receiving blood products the patient was sent to the radiology department for urgent CT angiography (CTA). Figure 15-1 Secondary aortoenteric fistula. (A) CT shows a small focus of air (arrow) adjacent to aortic graft. Note high-density material in distal small bowel and patent axillofemoral bypass graft in soft tissues of right anterior abdomen. (B) CT shows small “nipple” (arrow) at the distal aspect of the graft, which was later proven to be the site of the fistula. The infused CT study was performed with intravenous contrast only. An image through the lower abdomen revealed a small amount of air adjacent to the distal abdominal aortic graft and high-density hemorrhage filling bowel loops (Fig. 15-1A). The axillofemoral bypass graft appeared to be patent. A slightly caudal image showed a small “nipple” on the anterior and left lateral aspect of the graft. At surgery, this was found to be the site of an aortoenteric fistula (Fig. 15-1B). Secondary aortoenteric fistula. The patient was taken urgently to the operating room. The aortobifemoral bypass graft was removed en bloc, and the distal abdominal aorta was resected, and oversewn. The site of the enteric communication in the small bowel was resected, and the bowel was oversewn.
Clinical Presentation
Radiologic Studies
Diagnosis
Treatment
Discussion
Background
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


