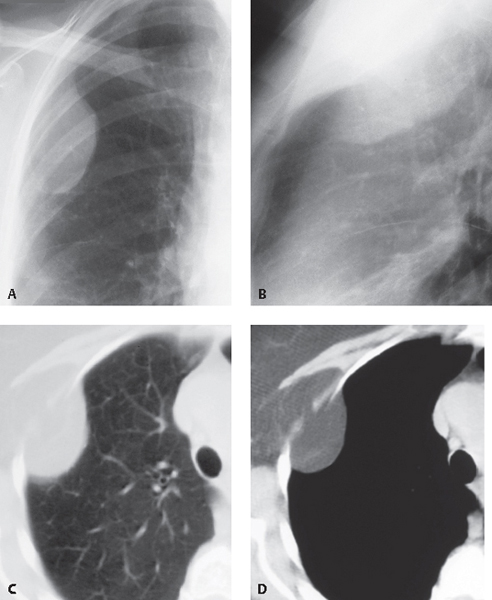
CASE 179 Asymptomatic 91-year-old woman Coned-down PA (Fig. 179.1A) and lateral (Fig. 179.1B) chest radiographs demonstrate a peripheral opacity in the right superior hemithorax that forms obtuse angles with the adjacent chest wall (Fig. 179.1A). There is discrepancy in margin visualization consistent with an extrapulmonary location. Contrast-enhanced chest CT (lung window, Fig. 179.1C; mediastinal window, Fig. 179.1D) shows a peripheral mass that forms at least one obtuse angle with the adjacent chest wall (Figs. 179.1C, 179.1D) and exhibits fat attenuation with scant thin linear soft-tissue elements (Fig. 179.1D). The mass is contiguous with subcutaneous fat attenuation tissue. Fig. 179.1 Chest Wall Lipoma None Benign chest wall tumors may originate from blood vessels, nerves, bone, cartilage, or fat. The imaging manifestations of benign and malignant chest wall lesions overlap, but some entities have characteristic imaging features that allow a confident diagnosis. Lipomas represent the most common soft-tissue chest wall tumors. They are well-circumscribed, encapsulated masses of adipose tissue that may lie deep within the chest wall and/or protrude into the thorax, displacing the pleura, mimicking other benign or malignant pleural lesions. The etiology of chest wall lipomas is unknown. Chest wall lipomas are typically incidental findings in asymptomatic patients. They occur most frequently in patients who are 50–70 years of age and are more common in obese individuals. • Well-marginated ovoid or lens-shaped chest wall mass (Figs. 179.1A, 179.1B) • Lesions may exhibit the incomplete border sign
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Findings
Chest Radiography
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


