PET imaging plays a vital role in the initial staging and post-treatment surveillance of patients with head and neck cancer. Although fluoro- d -glucose-PET remains the workhorse of PET imaging, novel tracers promise in being able to improve staging accuracy, refine radiation planning, and also provide tissue-specific diagnoses. Response assessment on PET may be accomplished using qualitative methods and by a variety of quantitative methods that have been validated in clinical trials. Simultaneous PET-MR is a promising technique, the implementation of which faces obstacles primarily related to cost, operation, availability, and lack of standardization of imaging techniques.
Key points
-
•
PET imaging plays a vital role in the initial staging and posttreatment surveillance of patients with head and neck cancer.
-
•
Awareness of pitfalls that lead to false positive and false negative image interpretation results is essential.
-
•
Baseline surveillance PET should be performed 3–6 months after treatment, as earlier imaging may show false positives. Liquid biopsy with ctDNA complements PET in HPV-positive head and neck cancer surveillance.
-
•
Neck Imaging Reporting and Data Systems is an easily applicable qualitative method for response assessment.
-
•
Simultaneous PET-MRI is a promising tool but its use is limited by availability, cost, patient comfort and lack of validation.
Abbreviations
| ACR NI-RADS | American College of Radiology’s Neck Imaging Reporting and Data Systems |
| AJCC | American Joint Committee on Cancer |
| CECT | contrast-enhanced computed tomography |
| CMR | complete metabolic response |
| CR | complete response |
| CT | computed tomography |
| ctHPVDNA | circulating tumor human papilloma virus DNA |
| EBV | Epstein-Barr virus |
| ENE | extracapsular extension |
| FDG | fluoro- d -glucose |
| FNA | fine needle aspiration |
| GTV | gross tumor volume |
| HNSCC | head and neck squamous cell carcinoma |
| HPV | human papilloma virus |
| IJV | internal jugular vein |
| NI-RADS | Neck Imaging Reporting and Data Systems |
| PD | progressive disease |
| PR | partial response |
| PERCIST | PET Response Criteria in Solid Tumors |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| SCC | squamous cell carcinoma |
| SUL | SUVs normalized by lean body mass |
| SUV | standardized uptake value |
| 3D-MIP | 3-dimensional maximum intensity projection |
Introduction
Head and neck malignancies arising from the upper aerodigestive tract account for over 65,000 new cases of cancer annually, representing about 3.5% of all newly diagnosed cancers in the Unites States. The vast majority is squamous cell carcinoma (SCC) and etiologic factors include alcohol and tobacco abuse and infection by human papilloma virus (HPV) and Epstein-Barr virus (EBV). In the United States, HPV accounts for 60% to 70% of newly diagnosed oropharyngeal SCC while EBV accounts for 95% of nasopharyngeal cancer.
This review will address the role of PET/computed tomography (CT) and PET/MR imaging in staging, treatment planning, and follow-up of these cancers. Given that the term head and neck squamous cell carcinoma (HNSCC) is an oversimplification of a process that can originate in diverse sites in the head and neck, with differing staging systems, management strategies, and prognostic implications, the scope of this article, will be necessarily broad. This review will largely restrict itself to 2-deoxy-2- 18 F-fluoro- d -glucose (FDG) PET, and the use of novel radiotracers will be addressed only briefly.
2-Deoxy-2-[ 18 F]-FDG has been the workhorse of nuclear oncology for several decades. 18 F, a positron emitter, is ideally suited for PET imaging due to its short positron range (maximum 2.3 mm and mean 0.5 mm) and short half-life (110 minutes). FDG is a glucose analog that after initial phosphorylation in the cell cytosol to 18 F-FDG-6-phosphate fails to proceed through the subsequent steps in glycolysis and becomes trapped in the cytosol until radioisotope decay (“metabolic trapping,” Fig. 1 ). Malignancies demonstrate increased glucose consumption (“Warburg effect”), including 18 F-FDG, through specific signaling pathways resulting in upregulation of facilitated glucose transporters (GLUT 1 and 3) and hexokinase (HK1 and 2) enzymatic activity. , The “Warburg effect” and “metabolic trapping” together make 18 F-FDG-PET a powerful tool for detecting malignancy.
18 F-FDG cellular uptake mechanism. 18 F-FDG, like glucose, is taken up by a cell through facilitated glucose transporters (GLUT 1 and 3 in particular). After conversion to 18 F-FDG-6-phosphate by hexokinase enzyme (the first step in the glycolytic pathway), the metabolite fails to proceed through the subsequent glycolytic steps and remains trapped in the cell until 18 F decay to 18 O. In malignant cells, the increased 18 F-FDG accumulation is aided by upregulated glucose transporters and enzymatic activity.
Staging head and neck squamous cell carcinoma
Primary Tumor Staging
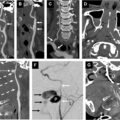
The T staging of primary HNSCC, according to the American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) staging manual, version 9, is determined through a combination of clinical examination, CT, and/or MR imaging. MR imaging is preferred if there is suspicion for skull base/intracranial/intraorbital invasion, perineural spread, or bone marrow involvement; to differentiate tumor from paranasal inflammatory disease; and if CT images are degraded by dental hardware artifact. CT is useful for assessing bone erosion/destruction. Although PET is highly accurate in the detection of primary tumors, its poor spatial resolution limits its clear delineation of tumor margins. False negative results from small superficial tumors and those located in/obscured by areas of high physiologic activity such as nasopharyngeal, palatine, and lingual lymphoid tissues. These areas may also give rise to false positive results. These errors may be ameliorated largely by obtaining contrast-enhanced CT (CECT) or MR imaging for attenuation correction. PET/CT may be useful in oral cavity SCC where dental artifact may limit precise T staging. SCC from an unknown primary tumor, presenting as cervical lymphadenopathy on clinical or imaging evaluation ( Fig. 2 A–D ) may account for 2.0% to 5.0% of all head and neck cancers. Unknown primary may be a transient definition with small primary tumors being often identified as HPV-positive oropharyngeal SCC. Its identification enables targeted treatment thus reducing treatment-related morbidity. Although PET/CT plays a key role in this regard, its accuracy is limited by the small size of these tumors and their presence in areas of intrinsically high metabolic activity such as the base of the tongue and palatine tonsils. Various studies have evaluated the efficacy of PET/CT in the detection of primary tumors with sensitivity ranging from 79.2% to 91.5% and specificity ranging from 70.4% to 87%. ,,
A 54-year-old man with right neck mass. Fine needle aspiration (FNA) showing keratinizing SCC. ( A , B ) Axial postcontrast CT shows no evident mass in the tonsillar fossae ( circles ) with a partially necrotic level II lymphadenopathy ( arrow ). Initial oral examination was negative suggesting occult primary. ( C , D ) Follow-up axial fused 18 F-FDG PET/CT show a focal asymmetrical uptake in right tonsillar fossa ( arrow in C ) suspicious for the primary site with metabolic activity in the metastatic right level II lymphadenopathy ( arrow in D ). Re-evaluation with direct laryngoscopy under anesthesia revealed a small ulcer in the right tonsillar fossa and biopsy was positive for SCC.
Nodal Disease
Staging of cervical nodal metastases in HNSCC incorporates nodal size, level, laterality, and extracapsular extension (ENE) of disease. This impacts treatment recommendations, with the goal of reducing overtreatment for HPV-positive patients with limited nodal involvement. A meta-analysis by Sun and colleagues revealed that pooled per-patient, per-neck-side, and per-neck-level sensitivities/specificities for 18 F-FDG-PET/CT were 0.91/0.87, 0.84/0.83, and 0.80/0.96, respectively. They concluded that 18 F-FDG-PET/CT has good diagnostic performance for the detection of regional nodal metastasis. PET is especially useful in the detection of nodal metastatic disease in the clinically/radiologically node negative (cN0) neck. A recent meta-analysis by Guedj and colleagues showed that 18 F-FDG-PET/CT has a high specificity and negative predictive value for ruling out nodal involvement in cN0 necks, but a limited sensitivity. It also revealed that 18 F-FDG-PET/CT missed nearly a third of cN0 patients who were found to be pN + upon pathologic analysis, suggesting that 18 F-FDG-PET/CT alone may be insufficient as a decision-making tool for elective neck dissection. The presence ENE is a poor prognostic indicator often necessitating chemoradiation and is more accurately detected by using CECT than PET/CT. It has been suggested that using a SUV max cutoff of 3.0 may provide appropriate diagnostic value in identifying ENE. ,
Distant Metastasis
Distant metastatic disease from HNSCC occurs in less than 5% of cases at initial presentation, usually to the lungs, liver, bones, and rarely to the brain. There are several factors that correlate with increased risk for distant metastasis at the time of initial staging and are summarized in Box 1 . Despite the presence of distant metastases portending poor outcome, the emergence of new chemotherapeutic and immunotherapeutic agents and local ablative techniques offers hope. FDG-PET is highly accurate in the detection of such spread, especially osseous metastatic lesions that may not be apparent on conventional imaging. Limitations include small metastatic lung nodules, which may require CT, and intracranial lesions that may be obscured by the intense physiologic uptake of brain parenchyma. PET/CT is also highly accurate in ruling out the presence of a second primary tumor, encountered in 5% to 10% of patients with HNSCC (especially in HPV-negative tumor and in smokers) with other upper aerodigestive tract and lungs being the most common sites of origin.
Box 1
Indications for 18 F-FDG-PET/CT in head and neck malignancies
-
Suspected head and neck occult primary:
-
•
No detectable primary malignancy on clinical examination or CT/MR imaging
-
•
-
Initial staging: In patients with risk factors for distant metastasis
-
•
High-grade tumor histology
-
•
Locally advanced primary cancer (eg, T3-T4)
-
•
Significant nodal disease in the neck (≥N1)
-
•
-
Treatment response:
-
•
Residual tumor evaluation after primary definitive treatment for locoregionally advanced disease
-
○
18 F-FDG-PET/CT is typically performed at 3 to 6 months after primary definitive treatment
-
○
-
•
Response to systemic therapy for diffuse distant metastatic disease
-
•
-
Surveillance:
-
•
Imaging interval is dictated by findings in posttreatment 18 F-FDG-PET/CT at 3 months
-
•
If PET/CT is negative and patient is asymptomatic at 3 months, then no further imaging is required; if positive at 3 months, then follow-up imaging or tissue sampling is indicated
-
•
Pitfalls with 18 F-fluoro- d -glucose-PET/computed tomography in head and neck malignancies
Interpretation of 18 F-FDG-PET relies on the visual observation of abnormal uptake above the surrounding background activity. However, depending on this single factor for detecting malignancy would introduce false negatives (tumor activity not being above the background) and false positives (nonmalignant activity being above the background). Appropriate interpretation of the PET findings would factor in the observations made on the concurrent CT, relevant prior imaging (both recent and remote), history and physical findings, and details about prior treatment. Common false-positive and false-negative PET findings in the head and neck region are summarized in Box 2 and depicted in Figs. 3–8 . The utility of standardized uptake value (SUV) is still debated, although it is routinely reported and denotes objectivity. Comparison of SUV of the index lesions following treatment and during follow-up is influenced by change in body weight, blood glucose level, injected dose, differences in the uptake time, and scanner differences. 18 F-FDG-PET/CT has low sensitivity for detecting brain metastasis because of the high physiologic background uptake in cortex and deep ganglia.
Box 2
False positives and false negatives encountered in head and neck cancer 18 F-FDG-PET/CT
Adapted from Boellaard R, Delgado-Bolton R, Oyen WJ, et al. FDG PET/CT: EANM procedure guidelines for tumor imaging: version 2.0. Eur J Nucl Med Mol Imaging 2015;42(2):328–54. https://doi.org/10.1007/s00259-014-2961-x . Epub 2014 Dec 2. PMID: 25452219 ; PMCID: PMC4315529.
-
False positives:
-
•
Physiologic uptake—lymphoid tissue of the Waldeyer’s ring, brown fat, masticator muscles, vocal cord uptake (especially if asymmetrical from palsy)
-
•
Artifacts—attenuation correction, misregistration
-
•
Inflammation—granulomatous and inflammatory lymphadenitis, infected benign cyst, odontogenic, sinusitis
-
•
Benign incidental tumors—Warthin’s tumor, thyroid adenomas, pituitary adenomas
-
•
Posttreatment—radiation-related inflammation, radiation-related osteonecrosis, immunotherapy-related inflammation
-
•
-
False negatives:
-
•
Suboptimal preparation—hyperglycemia/hyperinsulinemia
-
•
Patient factors—motion (voluntary, physiologic)
-
•
Small tumor size
-
•
Cystic tumors, necrotic lymph nodes
-
•
Low grade or mucinous tumors
-
•
A 62-year-old male with p16-positive SCC of left base of tongue ( asterisk ) with metastatic left level II lymphadenopathy ( red arrows ). ( A – C ) Axial fused 18 F-FDG PET/CT shows physiologic uptake in base of tongue ( yellow arrows in A ) and bilateral tonsils ( yellow arrows in B , C ), that can mimic or mask an underlying malignancy (false positive).
Posttreatment 18 F-FDG PET/CT on a 42-year-old man with p16-positive left tonsillar SCC with bilateral neck metastatic lymph nodes. ( A ) The 3-dimensional maximum intensity projection (3D-MIP) showing bilateral foci of intense uptake in lower neck ( red arrows ) and mild uptake in upper neck ( blue arrows ). ( B ) Axial fused PET/CT confirms residual activity of the metastatic nodes ( blue arrows ). ( C , D ) Axial fused PET/CT and noncontrast CT confirm the intense lower neck activity ( red arrows ) are false positive related to brown fat without visible lymph nodes.
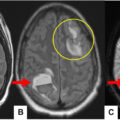
A 79-year-old man with cognitive decline underwent 18 F-FDG PET/CT for metabolic evaluation of the brain. ( A ) 3D-MIP, ( B , C ) axial fused PET/CT shows multifocal hypermetabolic lesions in bilateral parotid glands ( arrows ), suspicious for malignancy including lymphoma. A subsequent whole-body PET/CT was negative for disease elsewhere (not shown). ( D ) A review of a remote head CT from 8 years previously shows long-standing stability in the 1 cm left parotid gland deep lobe nodule ( red dotted circle ). A diagnosis of Warthin’s tumor (false positive for malignancy) was suggested given the bilaterality, multiplicity, stability, and intense FDG uptake.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


