Nasopharyngeal carcinoma (NPC) has a unique epidemiologic profile and a strong association with the Epstein-Barr virus. Radiologists should be familiar with the recently updated American Joint Committee on Cancer/Union for International Cancer Control version 9 staging system, effective January 1, 2025 and reviewed herein. NPC is usually treated with radiation and chemotherapy, with surgery reserved for persistent or recurrent resectable disease at the primary site or neck. Following primary treatment, patients typically undergo both clinical/laboratory and imaging surveillance, and radiologists should recognize recurrent disease and be familiar with the imaging appearance of treatment-related complications.
Key points
-
•
Nasopharyngeal carcinoma (NPC) has a unique epidemiology and close association with the Epstein-Barr virus.
-
•
MR imaging and 18F-fluorodeoxyglucose-PET/computed tomography are the mainstays of NPC staging given the proximity to the skull base/intracranial compartment and the propensity for metastatic disease.
-
•
As primary treatment of NPC is based on radiation and chemotherapy, primary staging is clinical (“c”) staging, rather than pathologic (“p”) staging.
-
•
Staging of NPC has been updated to the American Joint Committee on Cancer/Union for International Cancer Control version 9 as of January 1, 2025.
-
•
For radiologists, the most significant changes in staging are clarifications of T3 and T4 disease, the addition of advanced radiological extranodal extension as an N3 criterion and the subdivision of M1 into M1a/M1b.
Abbreviations
| ADC | apparent diffusion coefficient |
| AJCC/UICC | the American Joint Committee on Cancer/Union for International Cancer Control |
| ASL | arterial spin label |
| C | clivus |
| cEBV-DNA | circulating Epstein-Barr virus DNA |
| CPR | curved planar reconstruction |
| DCE | dynamic contrast-enhanced |
| DWI | diffusion-weighted imaging |
| EBV | Epstein-Barr virus |
| ENE | extranodal extension |
| FDG-PET/CT | 18F-Fluorodeoxyglucose-PET/computed tomography |
| H | Hypothalamus |
| HPV | human papilloma virus |
| ICA | internal carotid artery |
| LP | lateral pterygoid |
| M | Medulla |
| NP | nasopharynx |
| NPC | nasopharyngeal carcinoma |
| PBF | pharyngobasilar fascia |
| PMS | pharyngeal mucosal space |
| PPS | parapharyngeal space |
| PV | Prevertebral |
| RIS | radiation-induced sarcoma |
| RP | retropharyngeal |
| S | sphenoid sinus |
| T1WI | T1-weighted imaging |
| T2WI | T2-weighted imaging |
| TNM | tumor-node-metastasis |
Introduction
Nasopharyngeal carcinoma (NPC), the most common primary malignancy of the nasopharynx, has a skewed geographic distribution and a strong association with the Epstein-Barr virus (EBV). As treatment of NPC relies on radiation therapy and chemotherapy, assessment of disease burden and proper staging rely heavily on imaging. Staging of NPC has been recently updated by international consensus. An overview of NPC is presented herein with the intention of providing the radiologist with an understanding of the disease process and its updated staging system, as well as its treatment and associated treatment-related complications.
Epidemiology
NPC has a unique epidemiologic profile, with a high incidence in Southern China, Southeast Asia, North Africa/Middle East, and the Arctic– among these regions, Asian countries account for over 70% of the global burden. ,, There is a strong association with the EBV in such endemic areas, with genetically predisposed patients likely to develop NPC when exposed to additional viral and/or environmental factors. ,, In endemic regions, the association of EBV with NPC is often reported at 95% or greater, though one recent study found that 92% of cases were EBV+, while 7% were negative for EBV and positive for human papilloma virus (HPV); a small percentage were negative for both EBV and HPV, and even fewer were positive for both viruses. ,, This distribution differs in lower incidence, nonendemic regions where a higher percentage of patients may be positive for HPV or negative for both viruses. In North America, for example, a nonendemic region with a high prevalence of HPV+ oropharyngeal carcinoma, an HPV association is demonstrated in approximately 25% of cases of NPC, with HPV16 (44%) and HPV18 (33%) the predominant genotypes and with White patients overrepresented in this group.
Histology
NPC is a malignant mucosal epithelial neoplasm. The fifth edition of the World Health Organization Classification of Head and Neck Tumors recognizes 3 major histologic categories of NPC: keratinizing, nonkeratinizing, and basaloid SCC. Nonkeratinizing tumors can be further divided into undifferentiated and differentiated subtypes, both of which are strongly associated with EBV. The majority of EBV+ NPCs is both nonkeratinizing and undifferentiated, and conversely, the majority of nonkeratinizing undifferentiated tumors is EBV+. In nonendemic regions, keratinizing subtypes are more common, and the frequency of HPV infection is higher in keratinizing subtypes. ,
Circulating Epstein-Barr Virus DNA
The strong association of NPC with EBV makes circulating Epstein-Barr virus DNA (cEBV-DNA) a useful biomarker in EBV+ NPC, especially with advances in molecular biology and polymerase chain reaction techniques. Pretreatment cEBV-DNA levels are an independent prognostic factor for patients with NPC. During and immediately posttreatment, cEBV-DNA levels can be monitored, offering the possibility of early prediction of treatment response and deintensification. Patients with persistently detectable plasma EBV DNA following completion of definitive therapy have significantly worse survival outcomes than patients with undetectable EBV DNA. Following primary therapy, surveillance monitoring of cEBV-DNA may help to detect recurrent disease. Additionally, in endemic regions, cEBV-DNA can be applied to population screening.
Clinical Presentation
Clinically, NPC tends to affect middle-aged adults with a male predominance. Patients usually present with symptoms or signs referable to the primary site or to nodal metastatic disease, as spread to cervical lymph nodes is common in NPC; uncommonly, NPC may be detected incidentally on an imaging study performed for another indication, or a patient may present with symptoms or signs related to metastatic disease. Neck masses are the most common presentation, occurring in 60% to 70% of patients, followed by nasal symptoms (epistaxis and nasal obstruction), otological symptoms (hearing impairment, ear fullness, and otalgia), and cranial nerve palsies, as well as nonspecific symptoms such as headache.
Normal nasopharyngeal anatomy
Anatomically, the nasopharynx represents the uppermost aspect of the upper aerodigestive tract. It is bounded superiorly by the skull base and inferiorly by the soft palate, anteriorly by the nasal choana and posteriorly by the craniovertebral junction ( Fig. 1 A–F ). Laterally, the nasopharynx has more complex anatomy, including the Eustachian tube orifice, torus tubarius, and fossa of Rosenmuller (also known as the lateral pharyngeal recess).
Nasopharyngeal anatomy. ( A ) Sagittal and ( B ) axial T1WI demonstrate the relationships of the nasopharynx (NP), with the nasal cavity anteriorly, soft palate ( solid white arrow ) inferiorly, and the sphenoid sinus ( S ) superiorly, clivus ( C ) posterosuperiorly, and C2 vertebral body posteriorly. The fat-filled parapharyngeal space (PPS, asterisks ) lies lateral to the nasopharynx, while the hypoglossal canal ( dotted arrow ) is posterior. ( C ) Zoomed axial T1WI demonstrates the right fossa of Rosenmuller ( dotted line ), pharyngobasilar fascia ( dotted arrows ), Eustachian tube orifice (1), torus tubarius (2), levator veli palatini muscle (3), and tensor veli palatini muscle (4), lateral pterygoid (LP) and prevertebral (PV) muscles. ( D ) Coronal T1WI demonstrates these relationships and shows V2 in foramen rotundum ( arrow ), the medial pterygoid muscle (MP), and the PPS ( asterisks ). ( E ) More posterior coronal T1WI shows foramen ovale ( arrow ) and V3 below the skull base ( double arrows ), as well as fat in the PPS ( asterisks ). ( F ) Postcontrast fat-suppressed axial T1WI shows normal mucosal enhancement in the nasopharynx. Also indicated are the right internal carotid artery ( dotted arrow ), internal jugular vein ( broken arrow ), medulla ( M ), and left hypoglossal canal ( solid arrow ).
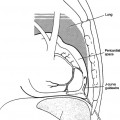
The nasopharynx is part of the pharyngeal mucosal space (PMS). The PMS is on the airway side of the middle layer of deep cervical fascia (buccopharyngeal fascia), and this fascia plus the adjacent pharyngobasilar fascia (PBF, the aponeurosis of the superior constrictor muscle) contribute to directing nasopharyngeal tumors superiorly toward the skull base, as the PBF attaches superiorly to the skull base medial to foramen ovale ( Fig. 2 A, B ). The PBF is, however, penetrated at the sinus of Morgagni, a gap in the fascial layer that permits the Eustachian tube and the levator veli palatini muscle to extend from the skull base to the nasopharynx, and this serves as a potential route for posterolateral tumor spread.
EBV+ NPC, with extensive erosion of the central skull base but without lateral extension. ( A ) Sagittal contrast-enhanced CT (CECT) shows an enhancing nasopharyngeal mass ( asterisk ) extensively eroding the clivus ( C ). ( B ) Coronal CECT shows a lack of tumor extension to the bilateral foramina ovale ( arrows ), as the tumor is directed superiorly by the strong pharyngobasilar fascia.
Imaging technique/protocols
MR Imaging
MR imaging is generally considered the technique of choice for imaging the primary site in NPC, due to its superior soft tissue resolution as compared with CT. , MR well demonstrates extension of tumor to the marrow space, adjacent soft tissues, and the intracranial compartment—it is particularly helpful for assessing extension of tumor to cranial nerves, Meckel’s cave and cavernous sinuses, and the meninges. MR coverage should extend from the superior orbit to the thoracic inlet to include the primary site and nodal basins. MR protocols typically include multiplanar T1-weighted imaging (T1WI), axial and/or coronal T2-weighted imaging (T2WI) with fat suppression, and postgadolinium T1WI with fat suppression, though fat suppression is not universally applied. NPC is typically isointense to muscle on T1WI, hyperintense to muscle and mildly hypointense to lymphoid tissue on T2WI, and enhances moderately and homogeneously postgadolinium ( Fig. 3 A–C ). , The appearance of NPC is similar whether the tumors are EBV+, HPV+, or virus-negative, though it has been suggested that HPV+ primary NPCs tend to be larger and more frequently originating from the center of the nasopharynx than their non-HPV counterparts, which typically arise laterally from the fossa of Rosenmuller or from the roof of the nasopharynx. MR imaging is also useful for assessing lymph nodes, though cervical nodal metastases may be MR-occult if they are small. Lymph node enlargement (short-axis diameter >10 mm in the neck, >6 mm in the retropharynx) and intranodal heterogeneity due to cystic and/or necrotic change are hallmarks of nodal metastases. Lymph nodes should also be assessed for advanced radiological extranodal extension (ENE, see later discussion).
Typical signal intensity of NPC on MR imaging appearance of NPC. ( A ) Axial T1 shows the tumor mass ( asterisk ) centered on the right fossa of Rosenmuller is isointense to muscle. ( B ) The tumor ( arrows ) is of intermediate signal intensity on fat-suppressed coronal T2WI, reflecting hypercellularity and high nuclear-cytoplasmic ratio. ( C ) The tumor ( asterisk ) enhances moderately and homogeneously on postcontrast fat-suppressed axial T1WI.
Advanced MR Imaging Techniques (Diffusion-weighted Imaging and Perfusion)
Diffusion-weighted imaging (DWI) is sensitive to the microscopic motion of water, which tends to be restricted in highly cellular processes such as tumors. NPC appears relatively hyperintense on DWI compared with surrounding normal soft tissue, and this can be helpful in identifying tumors and delineating their extent, as well as identifying tumor-involved lymph nodes. Additionally, quantitative information is available in the apparent diffusion coefficient (ADC), and changes in ADC may be helpful in predicting tumor response to treatment. Perfusion imaging is variably performed in NPC, but there is growing evidence in the literature that nongadolinium-based methods such as arterial spin label (ASL) perfusion or gadolinium-based methods such as dynamic contrast-enhanced (DCE) perfusion may be useful in characterizing primary tumors, assessing metastatic lymph nodes, predicting treatment response, and/or evaluating for persistent or recurrent disease after primary therapy ( Fig. 4 A–D ). ,,,
Advanced imaging of NPC. ( A ) The tumor ( arrows ) is conspicuous on DWI against a background of nondiffusion restricting and fat-suppressed normal tissues—it is similar in signal intensity to the medulla (m). ( B ) The tumor is relatively dark on ADC map (average ADC value 0.85 × 10 −3 mm 2/s). ( C ) The tumor is bright on ASL imaging, consistent with hyperperfusion. ( D ) DCE perfusion K trans map confirms hyperperfusion and increased permeability.
18F-Fluorodeoxyglucose-PET/Computed Tomography
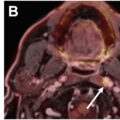
In a patient with an EBV+ neck node and an occult primary tumor, FDG-PET/CT may help to localize the primary site. While MR best characterizes the extent of an imaging-evident primary tumor, FDG-PET/CT is useful for assessing nodal metastatic disease and identifying distant metastases. Apart from retropharyngeal (RP) nodes, PET/CT has been reported to be more accurate than MR imaging for identifying cervical nodal metastasis and has been suggested to be the superior reference for neck status. FDG-PET/CT is also useful in target volume delineation/treatment planning, detection of residual/recurrent disease, and surveillance. Though FDG-PET/MR is not widely available, there is emerging evidence that this modality may be an effective initial staging procedure for NPC.
Tumor-node-metastasis staging of nasopharyngeal carcinoma
Accurate staging is essential for prognostication and for guiding treatment decisions in NPC, as well as for standardizing reporting of outcomes of treatment across centers. Staging is accomplished using the tumor-node-metastasis (TNM) system, which serves as a universal language for those involved in the care of patients with cancer. As of January 1, 2025, staging of NPC transitioned from the eighth edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) system to the ninth version. , The updated system has been shown to be superior to the prior in many important aspects, notably its outcome prediction accuracy and its balanced distribution. It should be noted that, as primary treatment of NPC is nonsurgical (see later discussion), initial NPC staging is based on clinical and imaging features, not pathologic staging. , Hence, the radiologist plays a key role in accurate TNM-categorization.
T Category
There are no substantive changes to the T category in AJCC/UICC9, but wording has been updated for T3 and T4 clarification. , T1 tumors are confined to the nasopharynx, or may extend to the oropharynx or nasal cavity, but they do not extend to the parapharyngeal space (PPS) ( Fig. 5 ). T2 tumors may extend to the PPS or adjacent soft tissues (medial or lateral pterygoid muscles and prevertebral muscles) ( Fig. 6 ). T3 tumors must demonstrate “unequivocal” infiltration of bony structures (skull base, including the pterygoid structures; paranasal sinuses; and cervical vertebra), with bone erosion and/or marrow space infiltration on imaging studies ( Fig. 7 ). Demonstration of bony sclerosis alone on CT/MR is not considered a criterion for T3 disease. Lastly, T4 tumors are typically large and aggressive, with involvement of the intracranial compartment, cranial nerves, hypopharynx, orbit, parotid gland, and/or soft tissues beyond the anterolateral surface of the lateral pterygoid muscle ( Fig. 8 ). Cranial nerve involvement should be unequivocal radiologically and/or clinically, and inferior orbital fissure involvement is considered as orbital involvement. Because perineural spread and involvement of skull base foramina commonly occur with advanced nasopharyngeal tumors, the course of branches of the trigeminal nerve, particularly V2 and V3, should be scrutinized in assessing for T4 disease. T0 is an uncommon, special case in which no tumor is found in the nasopharynx, but a patient has cervical lymph node(s) that demonstrate EBV+ tissue consistent with NPC. ,
T1 EBV+ NPC. ( A ) The small nasopharyngeal tumor ( asterisk ) mildly expands the right fossa of Rosenmuller on axial T1WI. ( B ) Axial T2WI shows no extension of tumor beyond the nasopharynx. The right parapharyngeal space (PPS) and prevertebral muscle (PV) are normal. ( C ) Postcontrast fat-suppressed axial T1 shows mildly enhancing tumor expanding the right fossa of Rosenmuller compared with normal brightly enhancing mucosa in the left fossa ( arrow ). ( D ) PET/CT shows the small FDG-avid primary tumor ( asterisk ).
T2 EBV+ NPC, with left mastoid effusion. ( A ) Axial T1WI shows infiltration of left parapharyngeal fat by tumor ( asterisk ), compared to normal fat in the right PPS on either side of the tensor veli palatini muscle ( solid arrow ). Right pharyngobasilar fascia ( dotted arrow ) is intact, but left PBF is infiltrated and not well seen. ( B ) Fat-suppressed axial T2WI and ( C ) postcontrast fat-suppressed axial T1 demonstrate left PPS encroachment ( solid arrows ) and infiltration of left prevertebral muscle ( dotted arrows ) compared with normal right PV muscle. ( D ) PET/CT shows FDG-avid left nasopharyngeal mass extending to the left PPS, while the right PV muscle and PPS are uninvolved.
T3 EBV+ NPC, with left mastoid effusion. ( A ) Fat-suppressed axial T2WI shows a homogeneous tumor mass expanding the left fossa of Rosenmuller. ( B ) Postcontrast fat-suppressed axial T1 shows infiltration of prevertebral muscle ( solid arrow ) and left PPS ( dotted arrow ), indicating at least T2 disease. ( C ) Sagittal and ( D ) coronal T1WI show loss of normal marrow fat in the sphenoid bone ( solid arrows ) adjacent to the NPC ( asterisk ), consistent with unequivocal skull base involvement and upstaging the tumor to T3 disease.
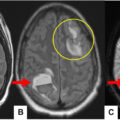
T4 EBV+ NPC in a patient with 2 years of epistaxis followed by headache, weakness, confusion, and right facial numbness. ( A ) Sagittal T1WI shows tumor ( asterisk ) infiltrating the clivus ( C ) and extending through the sella and suprasellar cistern to the hypothalamus (H), consistent with gross intracranial extension. ( B ) Postcontrast fat-suppressed sagittal T1WI shows diffuse moderate enhancement of the tumor. ( C ) Axial T1WI shows tumor in the right pterygopalatine fossa ( solid arrow ) and foramen rotundum ( dotted arrow ), consistent with gross cranial nerve involvement. ( D ) Coronal T1WI confirms right foramen rotundum/V2 ( dotted arrow ) and also right vidian canal ( solid arrow ) infiltration by tumor. Normal left foramen rotundum/V2 and vidian canal are indicated ( yellow arrows ).
N Category
Changes have occurred in the N category from AJCC/UICC8 to AJCC/UICC9. Compared with AJCC/UICC8, N0 to N2 categories have not substantially changed, though subcategory wording has been updated for clarity (see below) and to acknowledge the updated definition of N3 disease. , Previously, ENE was not considered in N categorization, but in AJCC/UICC9, advanced ENE has been added as an N3 criterion. “Advanced” radiological ENE connotes involvement of adjacent muscles, skin, and/or neurovascular bundle and corresponds to grade 3 image-identified disease. ,, As this has been shown to be an independent predictor of poor outcome, an absence of ENE has been added as a criterion for N0 to N2 disease, and presence of ENE advances the patient to N3. It should also be noted that less definitive findings of ENE (e.g. irregular/indistinct nodal margins, tumor extension confined to the perinodal fat, and/or matting of adjacent nodes) do not constitute advanced radiologic ENE. ,, Thus, for AJCC/UICC9, N0 continues to reflect no tumor involvement of regional lymph nodes. N1 reflects tumor involvement of unilateral cervical lymph nodes and uni- or bilateral involvement of retropharyngeal lymph nodes, with additional requirements of nodes ≤6 cm in greatest dimension, above the caudal border of the cricoid cartilage, and without advanced ENE ( Fig. 9 ). N2 encompasses tumor involvement of bilateral cervical nodes, as well as the additional requirements outlined for N1 disease ( Fig. 9 ). Lastly, N3 reflects unilateral or bilateral involvement of cervical lymph nodes as well as any of the following criteria: >6 cm in greatest dimension, extension below the caudal border of the cricoid cartilage, and advanced radiologic ENE as previously defined ( Fig. 10 ).
Fat-suppressed axial T2WI examples of N1 disease (patient 1, A, B) and N2 (patient 2, C, D) disease. ( A ) Enlarged right retropharyngeal node ( solid arrow ) compared to normal left node ( dotted arrow ). ( B ) Enlarged right level II node ( solid arrow ) compared to normal left nodes ( dotted arrows ). ( C ) Heterogeneous right level II node ( dashed arrow ) and enlarged left retropharyngeal node ( solid arrow ). ( D ) Multiple enlarged left level II nodes ( arrows ) without advanced radiological extranodal extension (ENE).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


