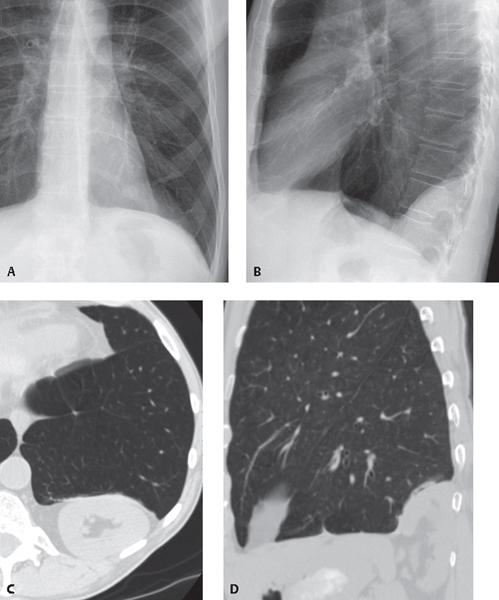
CASE 184 Asymptomatic 53-year-old man with a left posterior mass detected incidentally on chest radiography Coned-down PA (Fig. 184.1A) and lateral (Fig. 184.1B) chest X-rays show a well-defined mass in the posterior left inferior hemithorax that appears to abut the adjacent diaphragm. Contrast-enhanced chest CT (lung window) (Fig. 184.1C) and coronal reformation (Fig. 184.1D) demonstrate the well-defined mass abuts, elevates, and deforms the posterior aspect of the left diaphragm and contains the left kidney (Figs. 184.1C, 184.1D). Fig. 184.1 Bochdalek Hernia None Abdominal contents may herniate into the thorax through congenital or acquired diaphragmatic weak areas or through rents caused by trauma. Non-traumatic diaphragmatic herniation occurs most frequently through the esophageal hiatus and is usually related to obesity and/or pregnancy. Less commonly, herniation occurs through the pleuroperitoneal hiatus (Bochdalek hernia) or the parasternal hiatus (Morgagni hernia). Bochdalek hernias have been reported to occur more commonly on the left side, although a recent small series described a right-sided predominance (68%) with bilateral involvement in 14% of affected patients. Bochdalek hernias are associated with protrusion of omental or retroperitoneal fat that may be accompanied by abdominal organs, most often the kidney. Morgagni hernias
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


