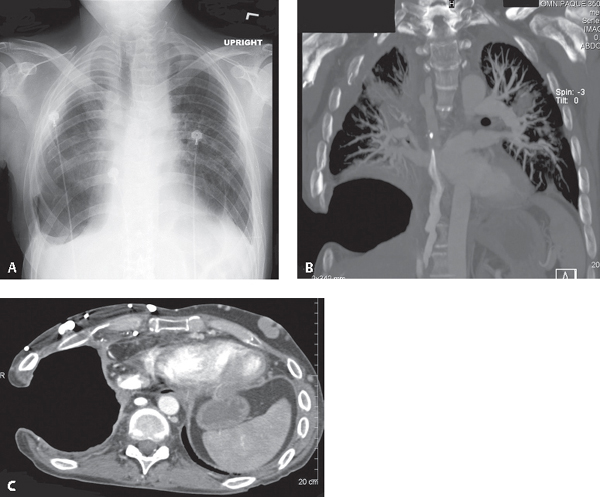
CASE 189 42-year-old man status post Eloesser pleurocutaneous window for chronic empyema PA chest radiograph (Fig. 189.1A) reveals partial surgical resection of the right eighth and ninth posterolateral ribs. A large air-filled cavity occupies the lower right thorax, communicating with the chest wall and outside environment. Contrast-enhanced coronal (Fig. 189.1B) (bone window) and axial (Fig. 189.1C) (mediastinal window) chest CT demonstrates the pleurocutaneous window to better advantage. The overlying ribs and associated intercostal muscles have been resected. Note the continuous epithelial lined parietal pleural surface of the permanent cavity. Eloesser Pleurocutaneous Window for Chronic Empyema Fig. 189.1 None Twenty to 60% of all cases of pneumonia are associated with parapneumonic effusions (PPE). PPE accounts for about one-third of all pleural effusions and is the most common cause of exudative effusion. Untreated or inadequately treated PPE may progress to empyema thoracis, which, by definition, is pus in the pleural space. If not drained, the effusion may become organized as fibroblasts grow into the pleural fluid from both the visceral and parietal pleura. This produces a thick inelastic pleural peel which prevents the lung from expanding, entrapping the lung. The key to successful treatment is evacuation of the infected pleural space and elimination of the dead space in the pleural cavity. However, the underlying pleural infection cannot be eradicated unless this peel is removed. Treatment options include: • Empyemectomy-decortication and open drainage • Pleurocutaneous window (Eloesser flap) • Muscle flap closure without pleural drainage Empyemectomy-decortication and open drainage are indicated for late Stage II (fibropurulent) or Stage III (chronic organizing) PPE with inadequate pleural drainage after tube thoracostomy and intrapleural fibrinolytic therapy. Decortication is preferred over open drainage. Pleurocutaneous window (Eloesser flap) is indicated for refractory pleural effusions (e.g., empyema, malignant effusions, esophagopleural fistulas) and creates permanent open access to the pleural space. Muscle flap closure without pleural drainage provides well-vascularized muscle tissue to close a bronchopleural fistula and obliterate the empyema cavity. • Pleural rind or peel with or without calcific pleuritis (Fig. 189.3) • Entrapment of the adjacent lung • Rib approximation and contraction of affected hemithorax
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Clinical Findings
Imaging Findings
Stage III Empyema
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


