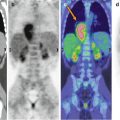
Fig. 3.1
(a) Maximal intensity projection showing focal 18F-FDG uptake in the mediastinum and right lung. (b, c) Axial CT and PET/CT fusion images show mediastinal uptake at the summit of the central venous line (b) and tracer stasis in the catheter reservoir (c)

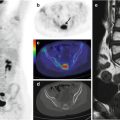
Fig. 3.2
(a) Axial CT and PET/CT fusion images show the axillary venous line (white arrow) and (b) focal mediastinal uptake at the terminus of the central venous line due to tracer stasis
Pediatric radiation dosimetry recommendations are contained in the ICRP guidelines, which identified the bladder wall as the critical organ for the effective dose received (range: 25.6–50.5 mGy varying on the basis of the body weight with a maximum administered FDG activity of 370 MBq for large-size children weighting ≥70 kg). In 18F-FDG–PET/CT, due to the high energy of photons emitted after tracer disintegration, radiation exposure to individuals accompanying the child must be considered. A good compromise is, for example, the presence of only one parent and not the child’s siblings during the uptake phase. The acquisition parameters of the CT scan should be tailored to the patient’s size. Those used in our center are 60–80 mA, 80–140 kV, and a helical pitch of 3.75:1. A 30–50 % reduction in exposure of the child patient relative to that of an adult will not cause an important loss of information. After the scan is completed, a fast review of the exam is recommended before the child leaves the scanning bed in order to avoid movements during the acquisition that can provoke the necessity to repeat it.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


