Axial T2WI at the level of lateral ventricles.
Axial FLAIR image at the level of lateral ventricles.

Leukoencephalopathy with Brainstem and Spinal Cord Involvement and Lactate Elevation
Primary Diagnosis
Leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation
Differential Diagnoses
Vitamin B12 deficiency
Spinal variant cerebrotendinous xanthomatosis
Adult-onset autosomal dominant leukodystrophy
Mitochondrial disorders
Imaging Findings
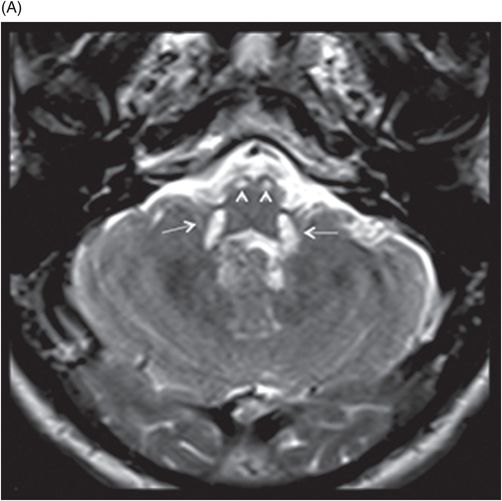
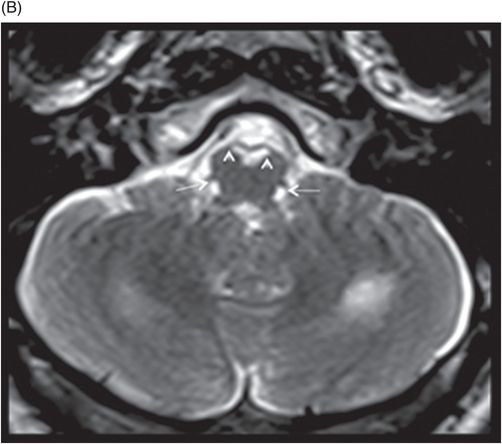
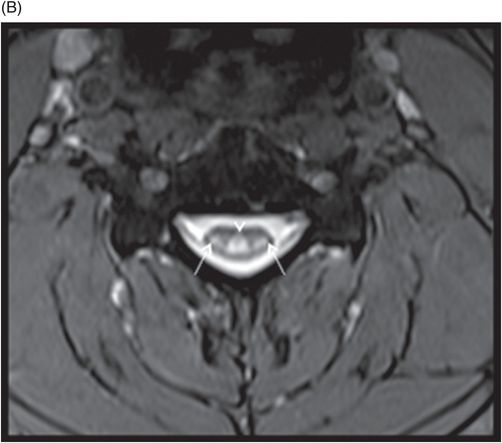
Fig 19.1: Axial T2WI and Fig 19.2: Axial FLAIR sequences showed diffuse and nearly symmetric hyperintense white matter changes in the bilateral periventricular regions with relative sparing of subcortical U fibers. Fig 19.3: Axial T2WI of the posterior fossa revealed hyperintense signal changes in the superior cerebellar peduncles (arrowheads) and intraparenchymal trajectories of trigeminal nerves (arrow). Fig 19.4: (A) Symmetric T2-weighted hyperintense signal changes were also noted in the inferior cerebellar peduncles (arrows) and pyramidal tracts (arrowheads) and along the decussation of the pyramid and medial lemniscus (B). Fig 19.5: (A) Sagittal T2WI of the upper thoracic spinal cord demonstrated linear, hyperintense signal changes with involvement of the posterior columns. (B) Axial T2WI of the same area demonstrated hyperintense signal changes in lateral corticospinal tracts (arrows) and posterior column (arrowhead). Fig 19.6: MR spectroscopy from the periventricular white matter shows an inverted doublet lactate peak at 1.3 ppm at TE 135 ms.
Discussion
The MRI findings of nearly symmetric involvement of the posterior limbs of internal capsule, pyramidal tract involvement, trajectories of the trigeminal nucleus, pyramidal involvement in the medulla, and signal changes in the dorsal and lateral corticospinal tracts are classic imaging features of leukoencephalopathy with brainstem and spinal cord involvement and lactate elevation (LBSL).
Although the spinal cord imaging findings mimic vitamin B12 deficiency, the brainstem imaging characteristics and negative hematologic tests for vitamin B12 deficiency exclude this as a diagnosis. Patients with the spinal variant of cerebrotendinous xanthomatosis also exhibit similar spinal cord imaging features; however, they present with a history of diarrhea, mental retardation, and cataract – which were absent in our patient. Tendon xanthomas are another clinical pathognomonic feature of this LBSL. Mitochondrial diseases tend to have varied brainstem imaging; however, involvement of specific areas of brainstem confirms a LBSL diagnosis. Adult-onset autosomal dominant leukodystrophy (ADLD) predominantly manifests with autonomic symptoms but can have similar diffuse supratentorial imaging findings and cord atrophy; however, the brainstem imaging features seen in this case are very characteristic for LBSL.
Mutations in DARS2, the gene encoding mitochondrial aspartyl-tRNA synthase, cause LBSL, an autosomal recessive disorder. Van der Knaap and colleagues first described LBSL in 2003. The disease begins in early childhood or adolescence, with gradually progressive cerebellar ataxia and motor and sensory neuropathy due to involvement of the dorsal columns and lateral corticospinal tracts. Seizures and cognitive decline that progresses to mental retardation are delayed features of the disease.
Based on MR imaging, the disease has major and supportive criteria. For imaging diagnosis of LBSL, all the major criteria and at least one supportive criteria have to be met along with high signal changes on T2-weighted MR images and low signal on corresponding T1-weighted images.
Major LBSL criteria
Homogeneous, spotty, or non-homogeneous white matter involvement with sparing of the U fibers
Lateral corticospinal tract and dorsal column signal abnormalities
Involvement of pyramids in the medulla oblongata






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


