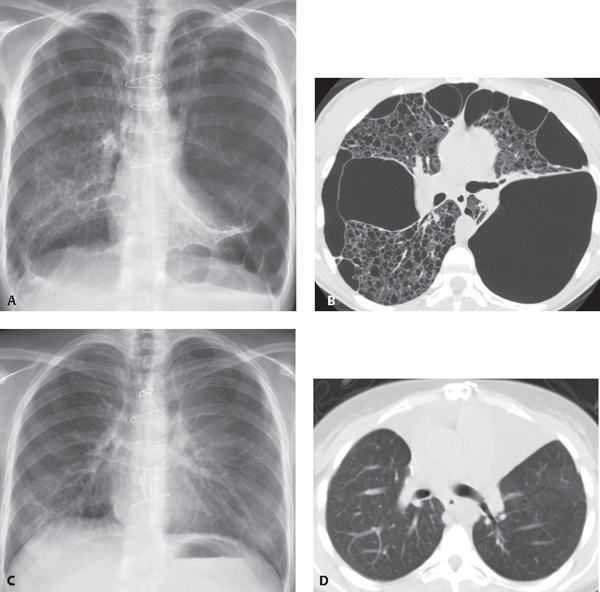
CASE 190 49-year old man with severe bullous emphysema before and after bilateral lung transplantation PA chest radiograph (Fig. 190.1A) demonstrates hyperinflation of the lungs with flattening of both diaphragms, and severe bullous emphysematous changes bilaterally. Post-surgical changes in the lungs and sternum were related to prior thoracotomy for resection of bullae. Unenhanced chest CT (lung window) (Fig. 190.1B) shows bullous emphysematous changes with giant bullae bilaterally. PA chest radiograph (Fig. 190.1C) following bilateral lung transplants reveals reduced lung volumes, normal bronchovascular structures, and improved configuration of both diaphragms. Unenhanced chest CT (lung window) (Fig. 190.1D) after bilateral lung transplantation demonstrates normal lung parenchyma bilaterally. Fig. 190.1 Bilateral Lung Transplantation None In recent decades, single and double lung transplantation have been established as successful treatments for advanced lung disease. Nearly 3,000 lung transplants were performed worldwide in 2009, according to the registry of the International Society for Heart and Lung Transplantation (www.ishlt.org). The most common indications for lung transplantation are emphysema/COPD, idiopathic pulmonary fibrosis (IPF), cystic fibrosis, α-1 anti-protease deficiency, and pulmonary arterial hypertension. Single lung transplantation has advantages in terms of extending treatment to more patients, since one donor may supply lung transplants for two individuals. But certain conditions require double (bilateral) lung transplantation. Patients with cystic fibrosis or severe bronchiectasis are at risk for suppurative lung infection in both native lungs, and thus double lung transplantation has been the preferred technique for those individuals. In recent years, single lobe transplants have been obtained from living donors. The morbidity and mortality associated with lung transplantation has decreased in recent decades, largely due to advances in surgical techniques. Bronchial connections may be established as end-to-end or telescoping anastomoses. The telescoping technique usually avoids the need for omental or intercostal muscle wrapping at the anastomotic site. Complications of lung transplantation may be categorized as early or late. The early complications
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


