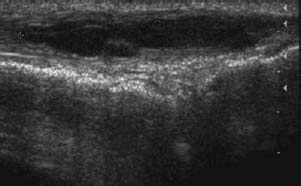
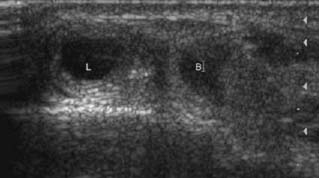
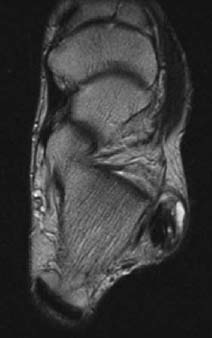
CASE 23 Anthony G. Ryan and Peter L. Munk A 26-year-old woman presented, having twisted her ankle playing tennis, with acute focal pain on the lateral aspect of her hindfoot just distal to the tip of the lateral malleolus. Figure 23A Figure 23B Figure 23C Figure 23D Figure 23E A sagittal ultrasound of the peroneus longus tendon (Fig. 23A) over the region of maximal pain and tenderness shows an irregular tubular anechoic collection within the peroneus longus tendon. Discontinuity of the internal fibrillar architecture is evident. Residual fibers are visible at the cephalad extent of the tendon (to the diagrammatic left of the image). The calcaneocuboid joint is visible deep to the tendon. Transaxial scanning at the same level (Fig. 23B) shows the tendons of the peroneus longus and brevis (labeled L and B) and an equivalent round anechoic defect within the substance of the peroneus longus. Transaxial T2-weighted images (Figs. 23C and 23D) through the same region show the tendon of the peroneus longus (anterolateral) to be 5 to 6 times the size of the adjacent tendon of the peroneus brevis. The internal architecture is disrupted, with a portion of normal (black) tendon visible on the deep/medial aspect and intermediate signal intensity rim surrounding an amorphous central higher signal component. The more caudad image (Fig. 23D) shows further disruption, including splitting of the tendon of the peroneus longus and high signal intensity fluid on the superficial aspect of the tendon. A coronal T2-weighted image (Fig. 23E) shows focal swelling and high signal intensity within the peroneus longus tendon. Deep to the obvious swelling, the normal peroneus brevis tendon is seen adjacent to the underlying calcaneus. Peroneus longus tear. None. The peroneal tendons are the principal everters of the ankle, coursing behind the lateral malleolus in a common tendon sheath, the latter extending to the level of the fibular tip. They run together in the retromalleolar fibular notch and are covered superiorly by the superior peroneal retinaculum, which resists tendon subluxation. In addition to ankle eversion, the peroneus longus is a flexor of both the ankle and the first digit (great toe). There are several acute bends on its course to the first metatarsal: at the retromalleolar fossa at the tip of the lateral malleolus, the peroneal tubercle of the calcaneus, and the cuboid notch. The tendons of longus and brevis separate at the peroneal tubercle, the latter serving to direct the peroneus longus tendon inferiorly and medially toward the cuboid notch. The bend at the cuboid notch coincides with the entry of the peroneus longus tendon to the plantar tunnel (cuboid tunnel) inferior to the cuboid bone. A fibrocartilage sesamoid, the os peroneum, is frequently present within the tendon at this site, protecting the tendon in its gliding motion over the peroneal tuberosity. The sesamoid is ossified in 20% of adults and, when present, is bipartite in 30% and bilateral in 60%. The peroneus brevis tendon everts the subtalar joint. It has two turns as opposed to the three of the longus, initially turning anteroinferiorly within the fibular groove at the tip of the lateral malleolus, with a second turn at the level of the peroneal tubercle, from which it courses anteriorly into its insertion at the base of the fifth metatarsal. As with injuries to other tendons, the presence of rheumatoid arthritis, diabetes, obesity increasing age, and hypertension all predispose to tendon tears. In younger patients, tears of the peroneal tendons typically occur secondary to sports involving a rapid change in direction (e.g., in soccer, tennis, and basketball), resulting in a longitudinal split as opposed to a transaxial tear. Avulsion fractures of the posterolateral fibula, such as in skiing, are occasionally complicated by disruption of the superior peroneal retinaculum. This leads to dislocation of one or both of the tendons. The peroneal tendons may also become entrapped between fragments of fibular or calcaneal fractures. The frequent bends, routes deep to retinacula and over osseous prominences, place the peroneal tendons at particular risk for the development of degeneration and tendinopathy, as well as subsequent tear as a “wear and tear” phenomenon. The peroneus brevis has a relatively greater predisposition to injury, however, as it is compressed to a greater extent between the more lateral peroneus longus and the stiff edge of the retromalleolar fibular notch. This compression predisposes the tendon to tendinosis, tenosynovitis, and consequent rupture. Tendinopathy at the level of its insertion on the fifth metatarsal is much less common. Peroneus brevis tendon tears are usually partial, in a longitudinal orientation, and centered at the tip of the lateral malleolus.
Peroneal Tendon Dislocation/Tear
Clinical Presentation


Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


