27 Osteoarthritis
Osteoarthritis can be induced by increased force on a normal joint or normal force on an abnormal joint (posttraumatic malalignment, chondropathy and/or osteopathy), as well as by constitutional factors. On the hand, osteoarthritis affects the proximal and distal interphalangeal joints (Bouchard’s and Heberden’s osteoarthritis, respectively), the carpometacarpal joint of the thumb, the scaphotrapeziotrapezoid (STT) joints, and the radiocarpal and midcarpal joints in the development of carpal collapse. Special manifestations are polyarthrosis, erosive osteoarthritis, and combined degenerative-rheumatoid arthritis. Predisposing factors are posttraumatic malalignments of bones and joints, chondrocalcinosis (CPPD deposition disease), hemochromatosis, and acromegaly. Initial stages of osteoarthritis can be sensitively determined with fine-focus radiography. CT arthrography and MR arthrography are most sensitive for detecting initial carpal osteoarthritis.
Pathoanatomy and Clinical Symptoms
Degeneration is the most common joint disease, with an exponentially increasing incidence after the age of 50 years. Osteoarthritis occurs with approximately the same frequency in males and females, with primary generalized polyarthroses and erosive subtypes being characteristic in females. Aside from the spine, the hips, and the knees, the joints of the hand are predominantly affected by degenerative osteoarthritis.
Osteoarthritis generally has both a predisposing and a triggering factor. However, a small group of primary joint degenerations occur without any plausible cause ( Table 27.1 ).
Increased pressure on normal articular cartilage:
|
Normal pressure on abnormal articular cartilage:
|
Diseases of the subchondral bone:
|
Cartilaginous damage as the initial stage of osteoarthritis results from the following pathophysiologic processes:
There is initially a defined edematous swelling of the articular cartilage.
Small tears then appear in the superficial layers of articular cartilage. If the deep layers break open, the cartilag progressively loses height until the subchondral bone is exposed.
Reactive synovitis with granulation tissue and neoangiogenesis sets in, probably as a result of cartilaginous particles that have been rubbed off. Joint effusion is usually only minimal and can appear suddenly.
Vascularization also occurs in the subchondral bone matrix, from which the deep layers of cartilage are vascularized during regenerative processes.
Diagnostic Imaging
Radiography
Conventional radiography is the basis of screening and follow-up of osteoarthritis of the hand, the radiographic criteria of which are summarized in Table 27.2 .
Aside from radiographic signs of the degenerative process, the wrists often reveal the causative factors of osteoarthritis, such as malalignment of the bones in carpal instability.
Computed Tomography
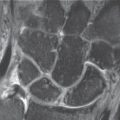
Due to its high spatial resolution with nearly isotropic voxels (Chapter 8), multislice spiral CT is currently best suited to identifying the initial signs of osteoarthritis at the wrist and also to determining its entire extent in advanced stages. Thin axial slices of 0.5–1 mm are recommended with an overlapping incremental reconstruction and multiplanar reconstruction (MPR), which completely captures the affected joints in different planes. In high-resolution CT, diagnostic criteria for osteoarthritis are asymmetries and narrowing of the joint space, defined cartilaginous defects ( Fig. 27.1 ), sclerosis and cysts in the subchondral bone plate, and carpal subluxations. A special application is CT arthrography (Chapter 8), in which the cartilage thickness and articular surface can be seen better than in MRI as a result of the high-resolution image matrix of 512 × 512.
Magnetic Resonance Imaging
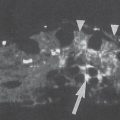
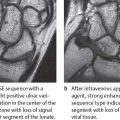
MRI is without doubt the procedure that provides the most thorough information concerning osteoarthritis because it provides information on signal intensity and morphology of the articular cartilage, as well as secondary changes in the subchondral bone plate. On the wrist and finger joints, however, where the articular cartilage has a thickness of only 1mm or less, MRI provides less information because of its limited spatial resolution. As explained Chapter 9, the following types of sequences are considered appropriate for examining the articular cartilage: fat-saturated protein-density (PD)-weighted FSE, T2*-weighted GRE, the multiecho data-image combination (MEDIC) hybrid sequence, the dual-echo steadystate (DESS) hybrid sequence, and fat-saturated 3D T1-weighted GRE. Early cartilaginous lesions can sometimes be recognized by a focal increase in signal intensity in T2-weighted sequences, and later chondropathic stages by irregular surface margins and reduced cartilage thickness. MR arthrography is useful for evaluating the morphology because the diluted contrast medium applied directly into the joint space separates the cartilaginous layers of the articular partners ( Fig. 27.2 ). Further MRI criteria are reactive areas of vascularization in the synovium and subchondral bone marrow, which are characterized by a significant contrast enhancement. Associated edema of the bone marrow appears hyperintense in T2-weighted sequences. Joint effusions occurring in erosive or activated stages of osteoarthritis also appear hyperintense in T2-weighted sequences.
|


Disease Entities
Osteoarthritis of the Finger Joints
Pathoanatomy and Clinical Symptoms
Osteoarthritis most commonly affects the proximal and distal interphalangeal joints, especially in women over the age of 45 years. Aside from a genetic disposition, no other causative factors for these degenerative forms are known (primary osteoarthritis). Only handedness and the extent of mechanical loading slightly influence the pattern of distribution and severity of degenerative changes. In addition to osteoarthritis of several finger joints, there are also degenerative changes at the radial side of the wrist, e.g., osteoarthritis of the scaphotrapeziotrapezoid (STT) and trapeziometacarpal (CMC I) joints. The other joints of the hand show no signs of degeneration.
Interphalangeal osteoarthritidis is usually painless. Joint function is maintained, except for morning stiffness and decreased grip strength. Soft-tissue nodules with mucoid contents (so-called mucoid cysts) arise on the dorsolateral aspect of the finger joints. These nodules communicate with the affected joint space and correspond histologically to ganglia. Arthrotic nodules on the proximal interphalangeal joints are called Bouchar nodules, and those on the distal interphalangeal joints are known as Heberden nodules, after the physicians who first described them.
Diagnostic Imaging
A typical sign of interphalangeal osteoarthritidis is the joint configuration. Since the condyle-shaped heads of the proximal and middle phalanges aremore resistant than the corresponding joint bases, in advanced stages of osteoarthritis a “seagull” deformity develops, with grinding down o the distal joint surfaces and a central spur remaining ( Table 27.3 , Fig.27.3 ).
Seagull deformities appear especially in erosive forms of osteoarthritis ( Fig. 27.11 ). They are also observed in hyperparathyroidism (see Fig. 31.8 ), in the final stages of rheumatoid arthritis (see Fig. 36.4a), and in psoriatic arthritis (see Fig. 37.2 ). Mostly, these diseases can be reliably differentiated by their different patterns of articular distribution and specific radiographic characteristics. In osteoarthritis, phalangeal subluxations to the radial or ulnar side are different from the palmar or dorsal deformities due to inflammatory tears of the tendons in rheumatoid arthritis.
|


Metacarpophalangeal (MP) joints II–V are seldom affected by degenerative changes in isolation ( Fig. 27.4 ). More frequent is the combination of advanced osteoarthritis in the interphalangeal joints with slight involvement in the MP joints – generally a narrowing of the joint spaces. In lesions of the MP joints resembling those of osteoarthritis, the following differential diagnoses must be considered:
The pattern of articular distribution in rheumatoid arthritis usually does not include the distal interphalangeal joints. There are also erosions, dislocations, and demineralization, but no osteophytes (see Fig. 36.3 ). The combination of rheumatoid arthritis with pre-existing Heberden nodules is possible, however.
Pronounced, hook-shaped osteophytes with flattening of the metacarpal heads and periarticular calcium deposits are typical of chondrocalcinosis (“pseudo gout,” CPPD deposition disease) and hemochromatosis (see Figs. 34.4 and 34.12 ).
Gout is typically manifested by means of marginal, cystic erosions and accompanying eccentric tophi with the density of soft tissues ( Fig. 34.1 ).
Wilson disease displays peculiar spicules.
Osteoarthritis of the Carpal Joints
Osteoarthritis of the Carpometacarpal Joint I (“Rhizarthrosis”)
Pathoanatomy and Clinical Symptoms
The trapeziometacarpal joint is a common location for degenerative changes, especially among women over 45 years of age. Clinically, the joint is swollen, and articular movement is accompanied by crepitation. Abduction and movements with axial pressure are painful. In advanced cases, there is a metacarpal subluxation to the radial and proximal aspects, resulting in consecutive adduction of the metacarpal I and hyperextension in the metacarpophalangeal joint. There is only a loose correlation between the clinical and the radiographic severity. Only half of the patients with osteoarthritis of the trapeziometacarpal joint have clinical symptoms.


Diagnostic Imaging
Radiographs of the wrist in two planes do not adequately depict the trapeziometacarpal joint. Because of the opposing position of the thumb in a palmar direction, the trapeziometacarpal joint can only be precisely visualized in the palmar-dorsal hyperpronated view (Chapter 1). This joint shows typical signs of osteoarthritis with narrowing of the articular space and increased subchondral sclerosis and osteophytes. The latter phenomena are more prominent on the trapezium than on the first metacarpal ( Figs. 27.5 , 27.11 ).
The classification shown in Table 27.4 is suitable for staging the severity.
Osteoproliferation in advanced osteoarthritis remodels the saddle shape of the trapezium joint surface into a half-cylindrical form. The joint surface of the trapezium is somewhat flatter in females, although there is no sex difference in the opposed joint surface of metacarpal I.
Stage | Radiographic Signs |
I |
|
II |
|
III |
|
IV |
|
|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


