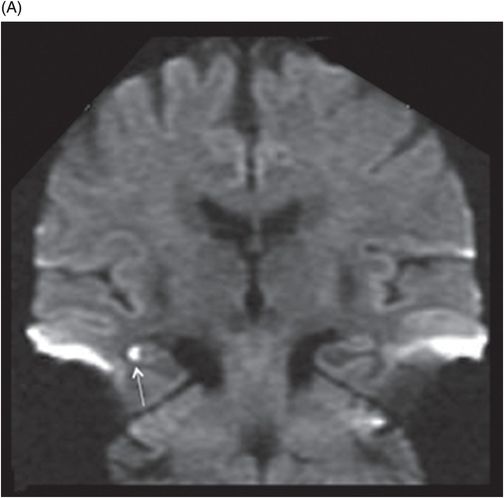
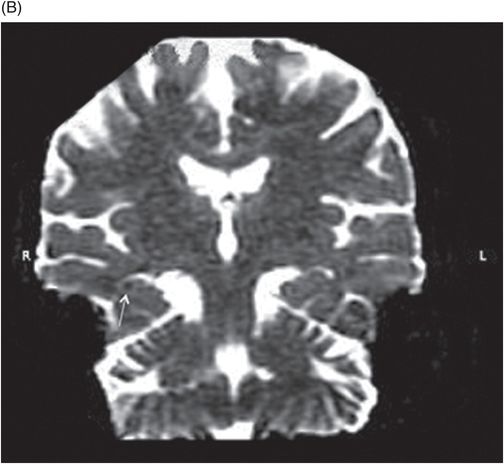
(A) Coronal DWI image at the level of the body of the hippocampi. (B) ADC image at the level of the body of the hippocampi.
Axial DWI image at the level of the temporal horns and hippocampi.
Coronal DWI MRI at the level of the body of the hippocampi (24 hours postadmission).
Transient Global Amnesia
Primary Diagnosis
Transient global amnesia
Differential Diagnoses
Acute confusional state
Complex partial seizure
Psychogenic amnesia
Korsakoff psychosis
Imaging Findings
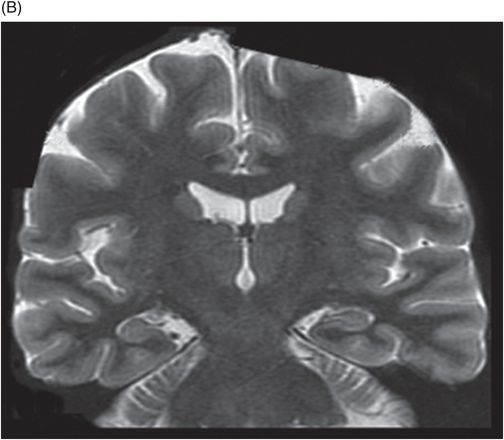
Fig. 28.1: (A) Axial T2WI and (B) coronal T2WI appear normal. Fig. 28.2: (A) Coronal DWI image demonstrated small focus of diffusion restriction in the body of right hippocampus (arrow). (B) ADC image demonstrated subtle changes (arrow). Fig. 28.3: Axial DWI image demonstrates technical limitations imposed by slice thickness; area of diffusion restriction is not visible. Fig. 28.4: Coronal DWI used for planning of axial image acquisition, however, clearly demonstrates area of diffusion restriction (arrow). Fig. 28.5: Follow-up MRI (24 hours postadmission) demonstrated complete resolution of previously noted diffusion restriction.
Discussion
The findings in the patient, including a small focus of diffusion restriction, acute-onset memory disturbance (anterograde amnesia), preserved cognition and attention span, and an intact personal identity with no neurologic deficits, typify the imaging and clinical findings suggestive of transient global amnesia (TGA).
The main points differentiating TGA from acute confusional state are the lack of attention capacity and the inability to maintain a coherent stream of thought – functions preserved in TGA patients. Similarly, a previous history of complex partial seizure or psychiatric condition may point to a different etiology. Psychogenic amnesia is usually seen in younger individuals and is associated with loss of personal identification, not found in patients with TGA. Typically, Korsakoff psychosis presents with prolonged anterograde and retrograde amnesia and usually there is an associated history of alcoholism.
Transient global amnesia is a heterogeneous clinical entity characterized by episodes of severe, sudden-onset, anterograde memory disturbances that last usually between 1 and 8 hours and usually resolve within 24 hours. Commonly, patients are described as confused but alert and attentive with preservation of higher-order cognitive skills. Patients remain fully communicative and often able to carry out complex tasks such as driving or playing music. During the amnesic episode, patients develop severe short-term memory loss and may repeat the same questions, usually related to orientation. On recovery, there is usually a complete return of anterograde and retrograde memory, with the exception of the transient amnesic episode, during which patients are unable to register any new memories.
Although exact etiology is unknown, there is consensus that brain areas involved include the medial temporal region and hippocampus. Transient ischemic attack, epilepsy, migraine, paradoxical emboli, venous congestion, and even jugular vein incompetency have been implicated as a cause for TGA. In support of a possible ischemic etiology, a few studies have reported small (< 5 mm) areas of restricted diffusion in the lateral hippocampal region. The number of diffusion-related abnormalities varies and ranges from 11.5% to 81%. This is likely related to multiple issues including imaging technique and plane of diffusion imaging, as well as the timing of the diffusion study. A significantly higher rate of detection of diffusion abnormalities has been noted in studies performed two to four days after symptom onset, as compared to the admission imaging. Higher resolution (2 mm vs. 3 mm slice thickness), higher b-values, and coronal orientation are thought to improve detection rate.
Brain lesions associated with TGA can be unilateral, involving either side of the brain, or bilateral (up to 50%), and multiple. The lateral hippocampus (CA1 region) has been shown to be involved in up to 94% of TGA cases, with no long-term residual structural changes. Another study, however, demonstrated the presence of hippocampal cavitary lesions that suggest late neuronal loss. Patients with TGA usually have lower prevalence of cerebrovascular risk factors as compared to stroke patients, with a lower recurrence rate and better prognosis.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


