Fig. 5.1
Images obtained with 3D ultrasound in which the surface renderization enables us to obtain coronal, oblique, and sagittal planes of normal fetuses with gestational ages between 27 and 33 weeks
5.2.2 Profile Views
In the profile view we study:
- 1.
The forehead (elusive or convex) and discard prefrontal edema (Fig. 5.2).
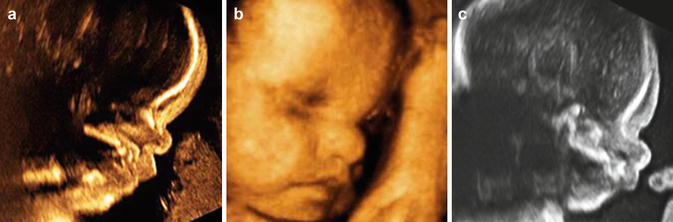
Fig. 5.2
Different pathologies assessed in the fetal profile. (a) 2D ultrasound of achondroplasia at 33 weeks; (b) 3D ultrasound of a 35 week fetus with severe cerebral ventriculomegaly (35 weeks); (c) 2D ultrasound of a fetus with Cornelia de Lange syndrome with Long and prominent philtrum, prefrontal edema, and retromicrognathia
- 2.
The nasal root (hypoplastic or very prominent) (Fig. 5.3).

Fig. 5.3
2D ultrasound of a fetus with Binder phenotype. Combination of abnormalities that are characteristic, such as underdevelopment of the middle third of the face; absence of the frontal-nasal angle with flattening of the glabella and verticalization of the nasal pyramid. The nose is short with flattened dorsal and nasal tip and shortened columella; prenasal hypoplastic maxilla with acute angle nasal lip and convex upper lip (Courtesy of Dr. Nerea Maiz Elizaran, Spain)
- 3.
The size of the chin (micrognathia and/or retrognathia) (Figs. 5.4 and 5.5). The mandibular disorders have been traditionally diagnosed by subjective evaluation of the chin in the profile study. In an attempt to use objective measures, Rotten et al. [4] described two indices to help diagnosis; the inferior facial angle (IFA) and the ratio of “mandibular width (MD)” and “maxilla height (MX)”. The IFA is obtained in a midsagittal plane of the face tracing a line perpendicular to the forehead at the level of the union of the two nasal bones. The second line links the more anterior portion of the lips and the extremity of the chin. The mean value of this angle is 65.5° and values below 49.2° are considered retrognathia.

Fig. 5.4
Surface renderization with 3D ultrasound of a fetus of 15 weeks, with retrognathia/micrognathia
Fig. 5.5
(a) 3D ultrasound of the face of a fetus of 34 weeks with retrognathia/micrognathia; (b) 2D ultrasound of the fetal profile in which the measured lower face angle is 47.06 (normal defined as >49.2°) [4]; (c) 3D ultrasound surface rendering of the axial plane with the “flipped face” technique; the hard palate is very short and small (highlighted in pink). The newborn presented with obstruction of the airway due to the abnormal location of the tongue; absence of the soft palate was diagnosed postnatally
- 4.
The philtrum (located between the columella that separates the nose and the upper lip) (Fig. 5.2c).
- 5.
The ears. The size needs to be compared with the published nomograms. The evaluation of the position must be carefully performed because an abnormally positioned ear can present in very subtle fashion, and the gestational age needs to be taken into account (Fig. 5.6).
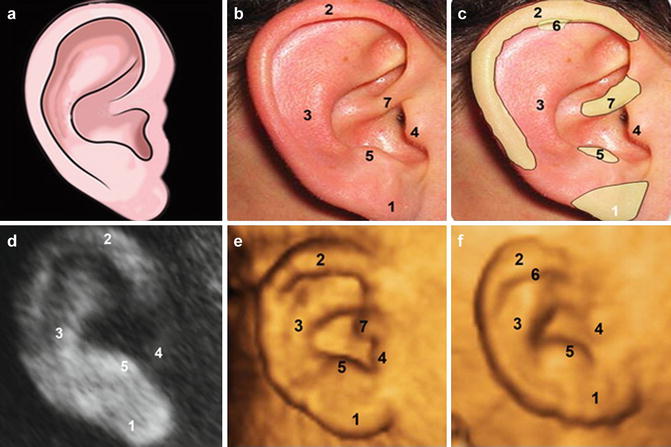
Fig. 5.6
(a–c) Outline and ear of a newborn showing different components; (d) fetal ear view with 3D ultrasound; (e, f) fetal ear with 3D ultrasound surface renderization; 1 lobe, 2 helix, 3 antihelix, 4 trago, 5 antitrago, 6 auricular tubercle, 7 cross of the helix
5.2.3 Coronal Views
In the coronal plane we assess:
- 1.
Orientation and size of the palpebral fissures
- 2.
Hypertelorism or hypotelorism (Fig. 5.7)

Fig. 5.7
Frontal-nasal dysplasia with nose involvement and hypertelorism. (a) Coronal plane with 2D ultrasound showing the intraorbital distance greater than the transverse diameter distance of each orbit. (b) Image with 3D ultrasound with renderization showing the dysplasia at the level of the nose. (c) Newborn
- 3.
Microphthalmia or anophthalmia (Fig. 5.8)

Fig. 5.8
Right lip-palate cleft with right microphthalmia. (a) Evaluation using the “reverse face” technique of the coronal plane; microphthalmia (arrow) and the affected secondary palate (curved arrow); (b) 3D ultrasound, high axial plane in which the arrow highlights the small right orbit, and without lens. (c) Fetal MRI; coronal plane showing affected orbit
- 4.
Shape of the nose
- 5.
Microstomia or macrostomia
- 6.
Tongue (possible macroglossia) (Fig. 5.9)

Fig. 5.9
Macroglossia in Down syndrome. It is “relative” macroglossia in that the tongue protrudes beyond the surrounding alveolar ridge due to the hypoplasia of the lower third of the face that is present in this syndrome
- 7.
Lips (discard fissures)
Reference values have been published for the majority of these measurements (width of the eyelids, area of the ears, height of the front, size of the philtrum, etc.) [5].
5.2.4 The Rest of the Examination
The majority of syndromes have extrafacial abnormalities and, in particular, abnormalities of the extremities. The dysmorphology examination, hence, includes detailed analysis of the limbs (Figs. 5.10 and 5.11). The number of fingers and toes should be counted. A postaxial polydactyly of only one hand can have the same semiological value as polydactyly of the four limbs. In addition, we should look at the orientation of the fingers and toes and the number of phalanges. The diagnosis of syndactyly, although difficult, may be possible with 3D ultrasound. However, parents should also be counseled that abnormalities of the fingers/toes can occur as isolated malformations without severe clinical significance.
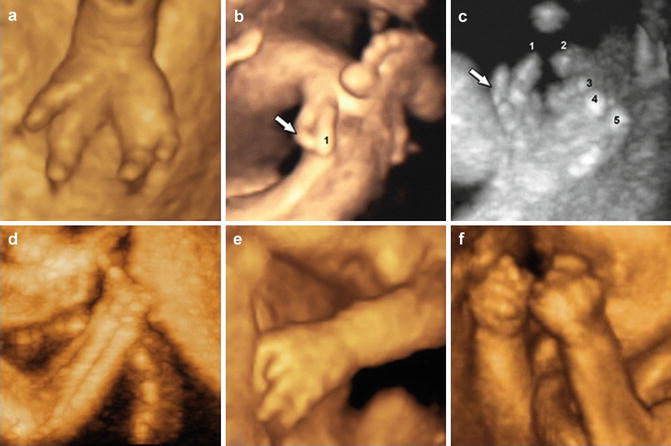

Fig. 5.10
(a) Surface rendering with 3D ultrasound of fetal hand with typical ectrodactyly (29 weeks). (b) Preaxial polydactyly. The extra finger (arrow) is encountered in the radial axis of the hand. (c) The same case as in (b) evaluated with 3D ultrasound in skeletal mode. Arrow showing the extra finger. (d) A typical ectrodactyly in a fetus of 33 weeks, 3D ultrasound in skeletal mode. (e) 3D ultrasound surface renderization: absence of first and second phalanges of the third finger. (f) “Claw hand,” superimposition of the fifth finger on the fourth and of the second on the third. Assessment with 3D ultrasound, surface renderization of a case of trisomy 18
Fig. 5.11
3D ultrasound surface rendering of abnormalities of the feet. (a) Postaxial polydactyly. (b) Club foot. (c) Metatarsus varus foot
5.3 Facial Malformation as a Sign of a Complex Syndrome
As we have commented, the analysis of the face forms part of the routine examination. It is necessary to emphasize the risk associated with performing a very detailed analysis of the face in the absence of a high level of suspicion of abnormality due to the precence of other abnormalities and/or family history. Many isolated dymorphology features may be encountered in normal individuals and should not be of concern to the parents. However, significant facial abnormalities (Figs. 5.12, 5.13, 5.14, and 5.15) can be the entry point for the diagnosis of fetal diseases and syndromes and can facilitate an overall fetal evaluation using the same criteria that we employ when we diagnose, for example, visceral malformations.



Fig. 5.12
Hypohidrotic ectodermal dysplaisa, a rare disease (1/10,000 to 100,000 newborns) caused by an abnormal development of the tissues derived from the ectoderm. These children have problems with the sweat glands, are incapable of sweating and, as such, have febrile confulsions. Further, they have thinning hair and hypoplasia of the dental arch with prominent lips and teeth that are pointed and separated. (a, b) Photographs of child affected with hypohidrotic ectodermal dysplasia. (c–e) 2D and 3D ultrasound performed prenatally showed the face to have very prominent lips and a small nose. (f) Newborn with the charactistic facial features of hypohidrotic ectodermal dysplasia [28]
Fig. 5.13
Partial trisomy of chromosome 20. Fetus assessed at 28 weeks showed shortened femur, slight ventriculomegaly with cephalic perimeter increased relative to gestational age, and hypoplasia of the nasal bones. The rest of the morphology assessment was normal. The karyotype showed a duplication of part of the material of the long arm of chromosome 20 (46 XY, dup (20) (q11.2q13.2). The child of 5 years of age has dysplasia of the corpus callosum, microcephaly, and moderate-severe mental retardation. (a) Hypoplasia of the nasal bones (arrow). (b) Facial profile obtained with 3D ultrasound surface renderization, showing the small nose but otherwise normal-appearing profile that would lead to a suspicion of trisomy 21. (c) Newborn [6]
Fig. 5.14
Cornelia de Lange syndrome. Rare syndrome (1/80,000 newborns) and sporadic, described by Cornelia de Lange in 1933. The syndrome has various characteristics, among which is a severe psychomotor delay. The fetus presents, at 26 weeks, micromelia in one arm with monodactyly and facial dysmorphism. There are no nasal bones and prefrontal edema is present; the nasal philtrum is very prominent due to excessive development of the upper maxilla. Micrognathia and retrognathia are present. The eyelashes (arrow) are long which indicate hirsutism; (a) and (b): in the assessment with 2D and 3D ultrasound, the philtrum is very large and prominent, with prefrontal edema and retromicrognathia; (c) and (d) show micromyelia of the arm with monodactyly in the assessment with 3D ultrasound, and following birth. (e) and (f) Eyelashes are extraordinarily long, an indication of hirsutism, as can be seen in the newborn [7]
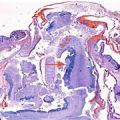
Fig. 5.15
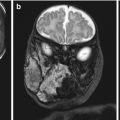 Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
 The Genetics of Facial Cleft
The Genetics of Facial Cleft
 Median Cleft Lip and Palate, Cutaneous Nasal Polyps, and Corpus Callosum Lipoma: A Case of Pai Syndrome Associated with Ventricular Septal Defects
Median Cleft Lip and Palate, Cutaneous Nasal Polyps, and Corpus Callosum Lipoma: A Case of Pai Syndrome Associated with Ventricular Septal Defects
 Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
 Micrognathia
Micrognathia
 Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face




Binder syndrome. (a) 2D ultrasound profile of the Binder phenotype with flat profile without nasal eminence. (b) 2D ultrasound showing a thick and striking femur due to calcification of the hypophysis, consistent with chondrodysplasia punctata associated with Binder syndrome. (c) Fetal X-ray showing asymmetry in the long bones and unilateral calcification of the epiphyses of the femur and humerus, as well as the vertebra-rib junction (Courtesy of Dr. Nerea Maiz Elizaran, Spain)
Related posts:
Congenital Subcutaneous Mixed Venous-Lymphatic Orofacial Malformation Associated with Macroglossia: Prenatal Diagnosis with Ultrasound and Fetal MRI
The Genetics of Facial Cleft
Median Cleft Lip and Palate, Cutaneous Nasal Polyps, and Corpus Callosum Lipoma: A Case of Pai Syndrome Associated with Ventricular Septal Defects
Acromelic Frontonasal Dysplasia (Median Cleft Face Syndrome)
Micrognathia
Magnetic Resonance Imaging (MRI) in the Evaluation of the Fetal Face
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
