Three-dimensional (3D) MR imaging has revolutionized musculoskeletal imaging by providing isotropic resolution and multiplanar reformatting, enabling high-quality reconstructions in any plane. Two-dimensional (2D) MR imaging has multislice acquisition with multichannel receiver coils; however, 3D sequences capture volumetric data in a single scan with equal voxel dimensions (typically 0.5–0.8 mm), allowing precise evaluation of intricate anatomy in structure-specific planes.. We review these advancements in detail, compare them to conventional 2D MR imaging, and highlight the advantages of 3D MR imaging in overcoming key limitations of 2D techniques for diagnosing hand and finger pathologies.
Key points
-
•
Among 3 dimensional 3D MRI techniques, 3D proton density-weighted fast spin echo (PDW FSE) isotropic imaging is ideal for internal derangements as compared to gradient-echo based or steady state MRI sequences.
-
•
The 3D PDW FSE sequence allows improved detection of partial and full-thickness small joint ligament injuries of the hand as compared to 2D MR imaging (level of evidence: III).
-
•
The 3D PDW FSE sequence depicts structure-specific reconstructions along the ligament or tendon axes for improved detection of their injuries and retraction.
Abbreviations
| 2 D | 2 dimensional |
| 3 D | 3 dimensional |
| DESS | dual echo steady state |
| DIP | distal interphalangeal |
| FDP | flexor digitorum profundus |
| FDS | flexor digitorum superficialis |
| FOV | field of view |
| FPL | flexor pollicis longus |
| fs | fat-suppressed |
| IP | interphalangeal |
| MCP | metacarpophalangeal |
| MIPs | maximum intensity projections |
| PDW | proton density-weighted |
| PDW FSE | proton density-weighted fast spin echo |
| PIP | proximal interphalangeal |
| RA | rheumatoid arthritis |
| RCLs | radial collateral ligaments |
| SNR | signal-to-noise ratio |
| STIR | short tau inversion recovery |
| T1W | T1-weighted |
| T2W | T2-weighed |
| TSE | turbo spin-echo |
| UCLs | ulnar collateral ligaments |
| VIBE | volume interpolated breath hold examination |
Introduction
Hand and finger structures have an intricate anatomy and are frequently injured in everyday activities and sports. ,, The fine anatomy of the hand and finger tendons, pulleys, cartilage, and synovial linings, and so forth requires high-resolution imaging for accurate diagnosis, since clinical examination is often challenging and diagnostically inaccurate due to similar presentations of different pathologies affecting these areas. While ultrasound provides high spatial resolution and real-time evaluation, MR imaging offers superior soft tissue imaging contrast and affords simultaneous assessment of both osseous and soft tissue structures. Conventional 2 dimensional (2D) MR imaging has been traditionally used for hand and finger imaging and is useful for various pathologies, like tumors, infections, and fractures. However, the ability of 2D MR imaging in evaluating fine or subtle internal derangements may be limited due to thick slices with large interslice gaps, which lead to decreased sensitivity and specificity. A potential alternative is 3 dimensional (3D) spin-echo MR imaging, which is now possible with high (0.5–0.8 mm) isotropic imaging resolution that allows multiplanar tissue plane-specific reconstructions. This article details the role of 3D MR imaging of the hand and fingers and compares it to 2D MR imaging.
Hand and fingers anatomy
The human hand is uniquely adapted for both strength and precision, requiring significant mobility for effective finger and thumb positioning, yet sufficient strength for grasping and delicacy for fine motor tasks. The hand comprises of 19 bones. Five metacarpal bones form the palm, articulating with each finger and the thumb at the metacarpophalangeal (MCP) joints. Each metacarpal bone features a head (proximal to the knuckle), shaft, and base (proximal at the wrist). Fingers consist of 3 phalanges (proximal, middle, and distal), which are connected by 2 interphalangeal (IP) joints, the proximal interphalangeal (PIP) joint and the distal interphalangeal (DIP) joint. The thumb uniquely has 2 phalanges and 1 IP joint. The wrist contains 8 carpal bones arranged in 2 rows. The proximal row, located dorsally near the forearm, includes the scaphoid, lunate, triquetrum, and pisiform. The distal row, closer to the palm, comprises the trapezium, trapezoid, capitate, and hamate. The wrist is formed by the articulation of the radius with the scaphoid and lunate.
The carpal tunnel is a narrow fibro-osseous passage bounded by the pisiform, hamate, scaphoid, and trapezium bones and covered by the transverse carpal ligament. It facilitates the passage of 9 tendons, 4 ligaments, and the median nerve from the forearm into the hand.
Collateral ligaments are situated on either side of each finger and thumb MCP and IP joints, preventing abnormal sideways movement. The volar plates are strong ligament, which connect the phalanges at palmar aspects of the MCP, PIP and DIP joints and prevent hyperextension during joint extension.
Each hand contains 34 intrinsic muscles. The thenar eminence controls thumb movement and includes 5 muscles: the interosseous, adductor pollicis, flexor pollicis longus (FPL), abductor pollicis brevis, and opponens pollicis. The adductor pollicis inserts on the ulnar sesamoid of the thumb, while the radial sesamoid anchors the abductor and opponens pollicis. The FPL tendon courses between these muscles and through the sesamoid interspace. The hypothenar eminence, located along the palm’s ulnar edge by the fifth digit, contains 3 muscles: abductor digiti minimi, flexor digiti minimi brevis, and opponens digiti minimi. These originate from the pisiform or hook of the hamate and control fifth digit abduction, flexion, and rotation toward the palm. The interossei, situated between the metacarpals, are responsible for finger abduction and adduction, comprising 4 dorsal and 3 palmar muscles. The 4 lumbricals originate from the radial side of the flexor digitorum profundus (FDP) tendons and insert into the radial side of the extensor expansions, flexing the MCP joints and extending the IP joints. ,,
The extensor tendons facilitate finger extension. They originate from the posterior forearm muscles, cross the dorsum of the wrist, and continue into the fingers, forming a flattened extensor hood at the MCP joint, stabilized by sagittal bands. The extensor mechanism fans out to attach to the phalanges: the central slip inserts onto the base of the middle phalanx, while the terminal tendon, formed by the fusion of 2 lateral tendons, inserts onto the base of the distal phalanx. Intertendinous connections, or juncturae tendinum, link adjacent extensor tendons over the dorsum of the hand, helping coordinate finger extension and providing additional stabilization. Contraction of extensor muscles pulls the tendon, straightening the finger. Flexor tendons, originating from forearm muscles, enable finger and thumb flexion. These tendons pass through the carpal tunnel and palm, bifurcating into 2 per finger. The flexor digitorum superficialis (FDS) attaches to the middle phalanx, flexing the MCP and PIP joints. The FDP inserts onto the distal phalanx, flexing the MCP, PIP, and DIP joints. These tendons are maintained close to the bones by a system of flexor pulleys. In the thumb, the FPL originates in the forearm and attaches to the distal phalanx, while the flexor pollicis brevis originates in the wrist and connects to the proximal phalanx. The flexor and extensor tendons of the hand are divided into 5 and 8 zones, respectively, based on their functional significance and implications for clinical management , ( Tables 1 and 2 ).
Table 1
Anatomic classification and clinical significance of flexor tendon zones in the hand
| Zone | Location | Clinical Significance |
|---|---|---|
| I | Distal to FDS insertion | Involves only FDP; injuries affect distal phalanx flexion and require precise repair for fingertip function |
| II | From FDS insertion to distal palmar crease | Contains both FDS and FDP within fibrous sheath; complex anatomy makes surgical repair challenging—historically called “no man’s land” |
| III | Palm region | Fewer pulleys and no sheath; better prognosis for tendon repair and fewer adhesions |
| IV | Carpal tunnel | Multiple tendons and median nerve in confined space; high risk of adhesions and nerve involvement postrepair |
| V | Forearm proximal to wrist | Often involves neurovascular structures; injuries may require microsurgical repair and carry higher morbidity |
Table 2
Anatomic classification and clinical significance of extensor tendon zones in the hand
| Zone | Location | Clinical Significance |
|---|---|---|
| I | Over DIP joint | Terminal extensor tendon; injury leads to mallet finger—requires splinting or surgical fixation |
| II | Middle phalanx | Lateral tendons; disruption may compromise coordinated extension |
| III | Over PIP joint | Central slip; injury may cause boutonnière deformity—early diagnosis and splinting critical |
| IV | Proximal phalanx | Less complex anatomy; good prognosis for surgical repair |
| V | Over MCP joint | Sagittal bands stabilize extensor tendons; rupture can cause tendon subluxation or snapping |
| VI | Dorsum of hand | Multiple tendons; accessible for repair with generally favorable outcomes |
| VII | Wrist level | Includes extensor retinaculum; high risk of adhesions and restricted motion postop |
| VIII | Distal forearm | Muscle-tendon junction; injuries may affect muscle contraction and require careful rehab planning |
Sensation and motor function of the hand are controlled by the radial, median, and ulnar nerves. The radial nerve courses along the radial side of the forearm, innervating the dorsal surface of the hand from the thumb to the third finger, including portions of the dorsal ring and middle fingers. The median nerve traverses the carpal tunnel and provides sensation to the thumb, index, middle, and half of the ring finger, as well as motor supply to the thenar muscles, except for the adductor pollicis brevis and deep head of the flexor pollicis brevis (which are innervated by the deep branch of the ulnar nerve). The ulnar nerve passes through Guyon’s canal, formed by the pisiform and hamate bones, where it divides into its main terminal branches, the superficial ulnar nerve supplying sensation to the little finger and half of the ring finger, and the deep ulnar nerve innervating many of the small intrinsic muscles of the hand including thumb adductors.
Conventional 2 dimensional MR imaging of the hand and fingers
MR imaging of the hand and fingers is commonly indicated for evaluating pain, swelling, injury, or limited range of motion. Underlying etiologies may include collateral ligament injuries, tendon and pulley injuries, osteochondral injury, and volar plate lesions. With its excellent soft tissue contrast and multiplanar, multiparametric imaging capabilities, MR imaging facilitates accurate localization and detailed characterization of abnormalities within this small and complex anatomy.
Using dedicated multichannel surface coils, high-quality images can be obtained using scanners at or greater than 1.5 T (Tesla). A combination of a strong gradient system with a small field of view (FOV) and thin slices improves spatial resolution with optimal signal-to-noise ratio (SNR) while reducing scan time. A small FOV (8–12 cm), matrix size of greater than 256 to 320, and 3 mm slice thickness with 10% gap are standard for optimal 2D imaging that allows in-plane resolution of 0.4 to 0.8 mm.
Patients are commonly positioned supine with the arm adducted close to the hip in mild supination. While the prone (superman) position (arm overhead, elevated, and elbow pronated) may offer advantages in fat saturation and reducing coil shine artifacts due to the hand being iso-centered within the magnet. Routine MR imaging of the hand and finger is performed in axial, sagittal, and coronal planes. Hand orientation in scans is typically in relation to the long axis of the third metacarpal of individual digits, depending on the area of interest, with finger orientation in relation to the MCP and PIP joints of the extended finger.
Generally, for internal derangements, one can obtain proton density-weighted (PDW) with or without fat suppression in axial and coronal planes. These are supplemented by T1-weighted (T1W) and fat-suppressed (fs) T2-weighed (T2W) or short tau inversion recovery (STIR) images for bone marrow assessment. Recently, intermediate-weighted T2W Dixon images have become available that produce several maps, including in-phase (IP), opposed-phase, and water images in similar resolution as PDW and fsPDW, obviating multiple sequence acquisitions in the same plane. In our practice, 3 plane simultaneous multislice acquisition T2 Dixons (SMS Dixon) in axial, coronal, and sagittal planes suffice for routine hand and wrist imaging. T1W and STIR images are added to infection, vascular malformation, and tumor protocols. The use of gadolinium contrast with T1W Dixons aids in the diagnosis and activity of arthritis, infection, and tumor pathology, and so forth. ,,
Three dimensional MR imaging of the hand and fingers
Three-dimensional MR imaging has become a transformative tool in musculoskeletal imaging, providing isotropic resolution, multiplanar reformatting, and comprehensive assessment of fine musculoskeletal structures. Unlike 2D MR imaging, which allows simultaneous multislice acquisition, isotropic volumetric 3D MR imaging sequences capture the entire volume in a single acquisition, with voxel dimensions equal in all 3 spatial directions—typically between 0.5 and 0.8 mm. This enables high-resolution imaging in any structural plane (axial, sagittal, coronal, curved, or oblique) without loss of image quality during reconstruction, offering flexibility for detailed diagnostic evaluation and for presurgical planning.
When combined with acceleration techniques, such as fast parallel imaging, scan times are significantly reduced to within 3 to 4 minutes. Compressed sensing or fast parallel imaging leverages mathematical reconstruction algorithms to produce high-quality images from undersampled data by exploiting the inherent sparsity of medical images. This approach maintains diagnostic image quality while shortening scan times, thus minimizing motion artifacts, and improving patient comfort. Advanced fat-saturation methods like Dixon and spectral attenuated inversion recovery (SPAIR) ensure uniform suppression across the FOV.
For imaging of the hand and fingers, the most commonly used sequences are 3D FSE or turbo spin-echo (TSE) sequences, marketed under names such as CUBE (GE, Waukesha, Wisconsin, USA), SPACE (Siemens, Erlangen, Germany), and VISTA (Philips, Best, Netherlands). These sequences are ideal for visualizing small ligaments, flexor pulleys, extensor mechanisms, and joint cartilage in structure specific planes. , While in-plane resolution of 3D MR imaging (0.7 mm) is slightly lower than 2D MR imaging, nongap volume imaging avoids partial volume artifacts, this producing real-black signal of normal or intact ligaments and connective tissue structures from the adjacent soft tissue edema or granulation tissue. Postcontrast 3D spoiled gradient-echo sequences like volume interpolated breath hold examination (VIBE) or VIBE-DIXON in 1.0 to 2.0 mm isotropic resolution are often employed to assess synovitis, tenosynovitis, or enhancing soft tissue lesions or tumors ( Figs. 1 and 2 ). These 3D Dixon-based sequences enhance fat suppression and are effective for evaluating marrow and soft tissue abnormalities. Since 3D sequences are quick, one can obtain perfusion imaging using 3D MR angiogram with sparse k-sampling volume acquisitions (like TRICKS-Time resolved imaging of contrast kinetics, TWIST- time-resolved angiography with interleaved stochastic trajectories, and 4D TRAK- Time-Resolved MR Angiography With Keyhole—different vendor-specific names) for the first 3 minutes using 10 seconds per frame with subtraction, maximum intensity projections (MIPs), and cine manipulations. The remaining 3 minutes are used for delayed postcontrast imaging using VIBE/VIBE Dixon with multiplanar constructions. Such postprocessed MIP images allow full extent of lesion detection by enhancing image signal and quality due to summation of SNR and contrast-to-noise ratio ( Fig. 3 ). These advantages render 3D MR imaging a powerful tool that can supplement or even replace conventional 2D sequences in routine clinical imaging for various pathologies. While gradient-echo based or steady state sequence-based alternatives are available like dual echo steady state (DESS), these are less desirable as compared to FSE variants due to superior resolution of the latter ( Fig. 4 ).
Active morphea-related synovitis and tenosynovitis—3D T1W FSE imaging of the hand: Contrast-enhanced sagittal ( A ), coronal ( B ), and axial ( C ) 3D T1W reconstructions reveal diffuse articular enhancements ( long arrows ) and tendon sheath synovial enhancements ( short arrows ) in this case of morphea.
Wrist-predominant rheumatoid arthritis (RA): Contrast-enhanced 3D T1W FSE imaging with coronal ( A ), sagittal ( B ), and axial ( C ) reconstructions display marrow edema of wrist bones ( short arrows ) and synovial thickening and enhancement ( long arrows ).
Wrist-predominant rheumatoid arthritis (RA): Three-dimensional time-resolved MR angiography with perfusion imaging: Coronal dynamic contrast-enhanced T1W FSE images of the hand ( A–C ) and respective MIP imaging ( D ) shows patent tortuous vessels and wrist synovitis with early arrival of contrast and persistence on delayed imaging.
High-resolution 3D MR imaging: The bone-on-bone osteoarthritis of the radiocarpal joint ( arrow ) detected on radiograph ( A ) is adequately depicted on the coronal 3D PDW FSE reconstruction ( C ), compared to less well depiction of 3D DESS image ( B ) ( arrows ). Also note better assessment of complete scapholunate tear on 3D PDS FSE ( small arrow ).
Advantages of three dimensional over two dimensional in various clinical scenarios
Osteochondral Plate and Articular Cartilage
Although full finger extension is the preferred position for optimal imaging, recent or prior injuries and soft tissue contractures often result in flexion or coronal plane deviation, which can compromise the quality of 2D MR imaging evaluation. Three-dimensional MR imaging enables multiplanar reconstructions aligned with the finger or target structure, facilitating precise evaluation of the osteochondral plate and articular cartilage. This enhances the resolution of hyaline cartilage, enabling more accurate diagnosis of cartilage injuries and informing treatment decisions between reconstruction and arthrodesis. In addition, osteochondral plate erosions may aid in distinguishing early arthritic changes from benign lesions, such as enchondromas, which typically preserve the articular surface.
Volar Plate
The volar plates (articular plates) are fibrocartilaginous structures, which are located on the palmar sides of the MCP and IP joints and play a critical role in the structural integrity and function of both the MCP and the IP joints, by reinforcing the joint capsules, cushioning the joints and limiting hyperextension. At the thumb MCP joint, the volar plate is situated between the 2 sesamoid bones and is closely associated with the FPL tendon. In the lesser MCP joints, the volar plate firmly attaches to the base of the proximal phalanx and, along with the accessory radial and ulnar collateral ligaments (UCLs), stabilizes the metacarpal head during flexion. The volar plate connects to adjacent volar plates via the deep transverse metacarpal ligament. At the IP joints, the volar plates are similarly anchored to the bases of the distal phalanges, providing anterior joint stability, preventing hyperextension, and contributing to the smooth gliding of flexor tendons. Volar plates are best visualized on axial or sagittal images, depending on joint positioning.
Volar plate avulsion fracture of the PIP joint is one of the most common hand injuries, which occurs due to sudden forced hyperextension and result in a bone fragment that is avulsed from the base of the middle phalanx. Partial or complete volar plate rupture without bone involvement can lead to joint instability or predispose the digit to chronic deformities, such as swan neck or pseudoboutonnière configurations. The decision for conservative management versus surgical intervention relies on determining the articular extent of avulsion fracture involvement and the degree of volar plate tear. ,
Two-dimensional MR imaging typically employs slice thicknesses of 3 to 4 mm and discrete planes. While it can detect edema, volar plate discontinuity, and associated avulsion fractures (such as those at the base of the middle phalanx in PIP joint hyperextension injuries), the sensitivity of 2D MR imaging is limited by slice thickness and partial volume effects. Small bony fragments or subtle soft tissue tears may be missed, especially if they fall between imaging planes.
In contrast, 3D isotropic FSE MR imaging eliminates interslice gaps and reduces partial volume averaging, thereby enhancing the detection of small avulsion fractures and permitting precise assessment of the tear size (such as partial vs complete tears) and its relationship to the adjacent structures using true-volar plate specific axial and coronal plane reconstructions ( Fig. 5 ). In addition, superior depiction of integrity or injury of hyaline cartilage and collateral ligaments facilitate presurgical planning as a one-stop shop.
Detailed 3D imaging of ligamentous injuries of the hand: In 2 patients with recent hand trauma, sagittal ( A ) and coronal ( B ) reconstructions of 3D sequences adequately depict tears of the volar plate ( A ) and the ulnar collateral ligament ( B ) of the first metacarpophalangeal joint.
Soft Tissue Mallet or Jersey Fingers
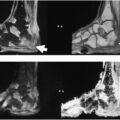
Forced flexion of an extended fingertip can stretch or tear the extensor tendon, and in some cases, avulse its insertion from the distal phalanx. This disruption in the extensor mechanism results in unopposed flexor pull, leading to the characteristic inability to extend the distal joint—producing the classic “mallet finger” deformity. The opposite of this phenomenon occurs with a jersey finger due to FDP tears. Differentiating between a soft tissue mallet or jersey injury and associated bony avulsion fracture, as well as accurately assessing the size of the fracture fragment, is essential for guiding treatment. For precise measurement of fragment size, non–fs 3D sequences are preferred, as they provide clearer cortical delineation, whereas fs 3D acquisitions are more suitable for detecting bone marrow or soft tissue injuries. Closed mallet fractures involving less than one-third of the articular surface and without DIP joint subluxation are typically managed nonsurgically with splinting. In contrast, surgical intervention is generally indicated for fractures involving more than one-third of the articular surface or those associated with joint subluxation.
Two-dimensional MR imaging acquiring images in discrete, fixed planes with interslice gaps is especially problematic when evaluating slender, obliquely oriented tendons like the terminal extensor or flexor tendons. Small or partial-thickness tendon tears may be missed or underestimated when the plane of imaging is not aligned precisely with the tendon’s long axis. Furthermore, terminal tendons in the hand and fingers are small and flat and intimately associated with adjacent subcutaneous structures. Standard 2D planes may not adequately capture the multiplanar trajectory of the tendon, resulting in an incomplete assessment due to partial volume and the tendon may appear abnormally hyperintense. Three-dimensional MR imaging allows excellent detection of normal or injured terminal tendons with higher reader confidence and diagnostic accuracy. , Specifically, a previous study demonstrated that 3D MR imaging improves accuracy in characterizing rotator cuff tear shapes compared with 2D MR imaging, while also enhancing reader confidence.
While the limitations of 2D sequences in assessing mallet finger injuries remain underexplored, existing studies involving the ankle and wrist joints have demonstrated the potential advantages of 3D techniques in detecting subtle ligamentous tears. These findings suggest that 3D sequences may offer enhanced diagnostic accuracy for small ligament injuries in anatomically complex regions, such as the DIP joint. , A prospective study comparing 2D MR imaging and 3D isotropic MR imaging for diagnosing anterior talofibular ligament injuries found that the sensitivity for detecting partial tears increased from 78% using 2D sequences to 83% using 3D sequences. This improvement was statistically significant ( P <.05), attributed to the enhanced ability of 3D sequences to provide more sections through the ligament, thereby offering better visualization of subtle injuries and reducing overlap artifacts in intact ligaments detecting partial tears increased from 78% using 3D sequences to 83% using 3D sequences providing more sections through the ligament and thus better visualization of subtle injuries or avoiding overlap artifacts with real-black signal of the fine ligaments when intact. A retrospective study showed that 3D FSE Cube sequences significantly outperformed 2D MR imaging in diagnosing partial anterior cruciate ligament tears. The sensitivity of diagnosis improved from 10% (2D) to 95% (3D), and overall accuracy increased from 79% to 86%. A comparative study involving rotator cuff tears demonstrated that thick slices and small gaps in 2D MR imaging cause partial volume averaging, which obscures small lesions. Conversely, 3D isotropic sequences reduce this artifact and allow multiplanar reformats from a single acquisition leading to improved diagnosis of partial extensor tendon tears ( Fig. 6 ).