There is a need for using standardized lexicons and risk-severity scoring systems in different disease conditions encountered in musculoskeletal (MSK) radiology for improved interdisciplinary care. Several radiology reporting and data systems (RADS) scoring schemes have been recently published in the last 5 years for bone tumors and other MSK conditions like soft tissue tumors, infections, and peripheral neuropathy. Such systems allow standardized radiology reporting and common language for interdisciplinary communications while facilitating timely and appropriate patient management. This article highlights the key points, advantages, and pitfalls in the usage and utility of various RADS systems available for MSK radiology.
Key points
-
•
MR imaging-based reporting and data systems (RADS) scoring systems allow improved radiology-pathology concordance and interdisciplinary communications for timely patient management.
-
•
Among various scoring systems for bone tumors, Osseous Tumor Reporting and Data System has been shown to exhibit highest accuracy and interreader reliability.
-
•
Soft Tissue Tumor Reporting and Data System, Neuropathy Score Reporting and Data System, and Musculoskeletal Infection Reporting and Data System are essential and validated systems for standardized risk and severity-stratification scoring of MSK conditions.
-
•
Used routinely, RADS scoring can allow longitudinal data collection for patient outcomes tracking and research across institutions.
Abbreviations
| ACR | American College of Radiology |
| ADC | apparent diffusion coefficient |
| BI-RADS | Breast Imaging-RADS |
| Bone-RADS | Bone Reporting and Data System |
| CT | computed tomography |
| DWI | diffusion-weighted imaging |
| HU | Hounsfield units |
| MSK | musculoskeletal |
| MSKI-RADS | Musculoskeletal Infection Reporting and Data System |
| NS-RADS | Neuropathy Score Reporting and Data System |
| OM | osteomyelitis |
| OT-RADS | Osseous Tumor Reporting and Data System |
| RADS | reporting and data systems |
| REST | Radiological Evaluation Score for Bone Tumors |
| SSR | Society of Skeletal Radiology |
| ST-RADS/ Soft tissue-RADS | Soft Tissue Tumor Reporting and Data System |
| WHO | World Health Organization |
Introduction
The field of musculoskeletal (MSK) radiology encompasses a broad spectrum of conditions that affect muscle, soft tissue, joints, and nerves, including infection, tumors, and trauma. As the clinical presentations of these pathologies and lesions are often nonspecific and variable, imaging plays an integral role in their diagnosis and guiding management. Timely and accurate diagnosis is critical in facilitating prompt appropriate treatment and minimizing complications that can have debilitating consequences for the patients.
Critical to the diagnostic process is a well-formulated report that utilizes consistent and standardized terminology and lexicons to describe the imaging findings. However, radiologists across different experience levels and institutions tend to use variable terminology to describe similar lesions. This is further exacerbated by the lack of widely accepted, standardized lexicons in MSK radiology, though some recent attempts have been made to address this fallacy. , Given the subjective nature of different words used in radiology reports and their variable meanings, several challenges exist for radiologists seeking to describe findings, diagnoses, and the severity of pathologies in a clear, straightforward manner that could aid clinicians in appropriately recommended and timely management. Thus, there is a need in the field of MSK radiology for standardized terminology and risk-severity scoring systems to facilitate more structured, consistent reports across different experience levels and institutions that can lead to proper interdisciplinary communications, appropriate recommendations for patient management, tracking of their outcomes, and longitudinal data collection for future secondary research.
In the last 5 years, several MSK-specific Reporting and Data Systems (RADS), inspired by guidelines like Breast Imaging-RADS (BI-RADS), have emerged to address this gap. However, the incorporation of these scoring systems into clinical practice has been sluggish. This can partly be attributed to the limited understanding of which RADS guidelines are currently available and which ones are best to use for different conditions as well as how to utilize them for standardized reporting. This article aims to discuss in detail the current RADS scoring systems for MSK conditions that have been validated and are available for clinical use, with illustrative examples to enhance the reader learning so that they can implement them in their practice.
Bone tumors
Primary bone tumors are rare neoplasms with variable features and clinical presentations that are estimated to account for less than 0.2% of all cancers. Of the malignant bone tumors, osteosarcomas are the most common with a bimodal peak incidence in adolescents and older adults. This is followed by chondrosarcomas in older adults and Ewing sarcomas in children and adolescents. , In 2020, the World Health Organization (WHO) published updated classifications for primary bone tumors based on histology and behavioral characteristics with further subdivision into individual tumor types. The histologic families of the WHO classification include chondrogenic, osteogenic, fibrogenic, vascular, osteoclastic giant cell-rich, notochordal tumors, hematopoietic, other mesenchymal tumors of the bone, and undifferentiated small round cell sarcomas of bone and soft tissue.
Given the rarity and variability of these bone tumors, radiologists play an instrumental role in diagnosis and management through the detection and clear description of these lesions on imaging. As such, standardized and structured imaging reports that are management-directed are paramount to facilitating timely workup. Currently, there are 4 major reporting systems for bone tumors: Bone Reporting and Data System (Bone-RADS), , Osseous Tumor Reporting and Data System (OT-RADS), Solitary Bone Tumor Imaging Reporting and Data System (BTI-RADS), and Radiological Evaluation Score for Bone Tumors (REST).
Bone Reporting and Data System
Bone Reporting and Data System for computed tomography and MR imaging
The Bone-RADS algorithms for computed tomography (CT) and MR imaging were published in 2022 by a Skeletal Society of Radiology (SSR) white paper committee for the diagnostic management of incidental solitary bone lesions identified. This committee, composed of 12 SSR members and 1 orthopedic oncologist with expertise in bone neoplasm imaging, was formed after the Practice Guidelines and Technical Standards Committee of the SSR highlighted the inconsistency in the diagnostic management of these incidental bone lesions in adults on CT and MR imaging. Bone-RADS proposes 4 categories based on possible diagnostic recommendations: Bone-RADS1—leave alone for benign lesions; Bone-RADS2—perform different imaging modality; Bone-RADS3—perform follow-up imaging; and Bone-RADS4—biopsy and/or oncologic referral for lesions with concerning features or that are at risk for pathologic fracture.
A total of 3 management algorithms were developed, with 2 for CT and 1 for MR imaging. The first CT algorithm focuses on “lucent” lesions, which were defined as lesions with greater than 90% of the volume having lower attenuation in Hounsfield units (HU) than normal trabecular bone (up to 200 HU). Lesions that meet the criteria of lucency, including cystic lesions and giant cell tumors, should then be evaluated with the proposed flowchart, which utilizes both clinical (pain, history of malignancy with high risk for bone metastases) and imaging (cortical involvement, soft tissue extension, pathologic fracture, and aggressive periosteal reaction) to determine a Bone-RADS category. The second CT algorithm is for “sclerotic/mixed density” lesions. “Sclerotic” lesions are lesions with higher density or 50% or greater attenuation than the surrounding trabecular bone while “mixed-density” lesions should contain an approximate one-to-one ratio of hyperattenuated and hypoattenuated areas relative to the adjacent trabecular bone; however, these 2 categories are combined into a single algorithm that serves essentially as a catch-all for any lesion that cannot be defined as a lucent lesion. As with the prior algorithm, the sclerotic/mixed density lesions are also evaluated using a combination of clinical and radiographic features to come to a final Bone-RADS determination. ,
The last algorithm is for lesions identified on MR imaging, with separate flowcharts based on t1-weighted (T1W) signal intensity. T1W hyperintense lesions are defined as having higher signal intensity than the surrounding skeletal muscle or intervertebral disc. The corresponding flowchart for these lesions primarily assesses MR imaging features, including level of hyperintensity relative to surrounding structures and signal changes on in-phase and out-of-phase chemical shift imaging. T1W isointense/hypointense lesions are characterized as lesions with signal intensity that visually appears the same or lower than that of the adjacent muscle or intervertebral disc. As most of bone neoplasms and metastatic lesions tend to fall into this category, further evaluation with characteristics of the lesion on T2 imaging is critical to differentiate between benign and more concerning lesions. For T2 hyperintense lesions, which are defined as having high signal intensity comparable to fluid, the algorithm recommends evaluating for a combination of clinical and imaging factors (concerning imaging features vs features characteristic of benign lesions like enchondroma). With regards to T2 hypointense lesions, like enostosis, hemosiderin-containing, fibrous lesions or osteoblastic metastases, determination of Bone-RADS classification is influenced by the presence of any concerning imaging features as well as prior history of malignancy.
The Bone-RADS classification system provides a set of easy-to-understand management-driven mutually exclusive algorithms for solitary incidental bone lesions that excel in characterizing benign lesions and ensuring more concerning and aggressive lesions receive appropriate further workup. The decision-tree approach is adaptable to both radiographic and clinical features of lesions, generating standardized and consistent imaging reports that can help guide clinical management. Recent clinical validations studies have also suggested the clinical utility of Bone-RADS. A recent study by Park and colleagues found the CT algorithms of Bone-RADS to have good sensitivities for assessing lucent (95% and 82% for each respective reader) and sclerotic/mixed density lesions (75% and 68%) with very good overall interreader reliability as well. However, specificities were found to be poor for both algorithms, ranging from 11% to 27%, with moderate accuracies of 42% to 57%, highlighting some of the limitations of the system. A subset of limitations may be attributed to the overemphasis on clinical features, such as pain, in the assessment process that may result in the classification of some benign lesions as Bone-RADS4 and thus receiving unnecessary workup. Furthermore, non-MSK radiologists may have a more challenging time identifying certain classic presentations of benign lesions on imaging, leading them to pursue additional, unnecessary workup as per the recommendations of the flowcharts. These conjectures are supported by a study performed by Haseli and colleagues, where a revised Bone-RADS classification system with reduced emphasis on clinical features such as pain and history of malignancy saw improved specificity and accuracy while maintaining good sensitivity. Other disadvantages of the Bone-RADS classifications include the lack of validation testing for the MR imaging algorithms, the arbitrary follow-up recommendations for Bone-RADS3 lesions (6, 6, 12 month intervals for 2 years), and the somewhat cumbersome nature of diagnostic approach and need to remember the algorithms. It is also note that Bone-RADS does not allow risk-severity scoring to differentiate benign from malignant lesions, follows a conservative approach toward not missing aggressive-malignant lesions, and is merely a tool for further management recommendation ( Fig. 1 ).
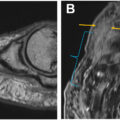
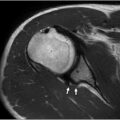
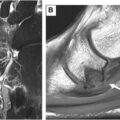
Coronal CT, T1W, T2W, postcontrast fsT1W, axial DWI, and ADC images in a young person with leg pain show a well-defined geographic lesion with sclerotic margins on CT, moderate enhancement, lack of peritumoral edema, and mild DWI restriction (ADC = 1.3–1.6) consistent with fibrous dysplasia. BONE-RADS = 4, OT-RADS = 2, BTI-RADS = 1.
Bone Reporting and Data System for radiographs
The Bone-RADS risk stratification system for bone lesions on radiographs was created in 2023 by a committee of experts assembled by the American College of Radiology (ACR). In this system, 5 radiographic features were identified to be predictive of malignancy risk: margination or zone of transition, pattern of periosteal reaction, depth of endosteal erosion, presence or absence of pathologic fracture, and presence or absence of soft tissue mass. Points are assigned based on each radiographic feature and then summed to determine a final point total that corresponds with a Bone-RADS score of 0 to 4, with Bone-RADS 1 characterizing very low risk and likely benign lesions to Bone-RADS 4 describing high-risk lesions that are highly suspicious for malignancy ( Table 1 ).
Table 1
Bone Reporting and Data System for radiographs
| Margin | Periosteal Reaction | Endosteal Erosion | Pathologic Fracture | Extraosseous Soft Tissue Mass | History of Primary Cancer |
|---|---|---|---|---|---|
| Geographic, well-defined lesions with marginal sclerosis (IA) = 1 | None = 0 | Mild = 0 | No = 0 | No = 0 | No = 0 |
| Geographic well-defined lesions without marginal sclerosis (IB) = 3 | Nonaggressive = 2 | Moderate = 1 | Yes = 2 | Yes = 4 | Yes = 2 |
| Geographic lesions with ill-defined margins (II) = 5 | Aggressive = 4 | Deep = 2 | — | — | — |
| Lesions with changing margins (IIIA), nongeographic margins (IIIB), or radiographically occult lesions with invisible margins identified by other imaging (IIIC) = 7 | — | — | — | — | — |
| Point Total | Bone-RADS Score | Description |
|---|---|---|
| N/A | 0 | Incompletely characterized |
| 1–2 | 1 | Very low risk—likely benign |
| 3–4 | 2 | Low risk—probably benign |
| 5–6 | 3 | Intermediate risk—potentially malignant |
| 7+ | 4 | High risk—highly suspicious for malignancy |
A major advantage of Bone-RADS for radiographs is that it provides a set of clearly defined algorithms created by a committee of experts with an associated standardized reporting template. It also serves as a useful risk-stratification tool with appropriate follow-up management recommendations to aid clinicians in the decision-making process. However, some of the shortcomings of Bone-RADS for radiographs include the lack of clinical testing data to support the utility of the system in clinical practice, the use of radiographs as the only imaging modality, and not using tumors as per standardized classifications such as the WHO classification of bone lesions.
Osseous Tumor Reporting and Data System
OT-RADS was developed in 2021 for differentiating benign and malignant bone tumors on MR imaging by a team consisting of 5 radiologists, 1 oncosurgeon, and 1 methodologist based in the University of Texas Southwestern Medical Center. Inspired by BI-RADS, this reporting system delineates 7 quantitative categories for bone tumors based on the WHO classification with associated management recommendations and likelihoods of malignancy ( Table 2 ). Each classification includes not only imaging features of the lesions on typical MR imaging sequences, but also on diffusion-weighted imaging (DWI) and associated apparent diffusion coefficient (ADC) maps.
Table 2
Osseous Tumor Reporting and Data System
| Classification | Category | Management | Likelihood of Malignancy |
|---|---|---|---|
| OT-RADS 0 | Incomplete imaging | Recall for additional imaging/await prior examinations | N/A |
| OT-RADS I | Negative | No further imaging follow-up | Essentially 0% |
| OT-RADS II | Definitely benign | Follow up as per clinical team recommendations | Essentially 0% |
| OT-RADS III | Probably benign | Follow-up in 3 mo, 6 mo, 1 y, and 2 y, or <2 y/shorter term follow-up is adequate if lesion resolves or significantly regresses | Less than or equal to 2% |
| OT-RADS IV | Suspicious for malignancy or indeterminate | Tissue diagnosis or short-term follow-up in 4–6 wk. If indeterminate or negative on tissue sampling, further follow-up similar to OT-RADS III | More than 2% and <50% |
| OT-RADS V | Highly suggestive of malignancy | Tissue diagnosis | More than or equal to 50% |
| OT-RADS VI | Known biopsy-proven malignancy or recurrent malignancy in the tumor bed | Surgical excision or further treatment as clinically appropriate | N/A |
OT-RADS 0 describes nondiagnostic or incomplete studies. OT-RADS I is used if no lesion is identified. OT-RADS II describes lesions that are definitely benign, such as simple bone cyst, lipoma, nonossifying fibroma, fibrous dysplasia, and osteoid osteoma. On postcontrast MR imaging, these lesions have either no enhancement, thin (<2 mm) peripheral and/or septal enhancement, nidus-like enhancement (as with osteoid osteomas), or variable enhancement. Associated DWI would exhibit moderate hyperintensity on both DWI and ADC images with T2 shine-through effects and mild ADC restriction (see Fig. 1 ). OT-RADS III describes bone tumors that are probably benign and associated with 2% or less malignancy (low-risk). Osseous tumors that fit within this category include intraosseous myxoma, classic giant cell tumor, chondroblastoma, Paget disease, and so forth. Postcontrast MR imagings typically show variable enhancement. OT-RADS IV describes indeterminate, potentially malignant tumors with a 2% to 50% (intermediate) risk of malignancy. On MR imaging, these lesions may appear to have mixed intensity or solid features with variable enhancement on postcontrast sequences. Examples of these tumors include osteoblastoma, atypical cartilaginous tumor, and grade I chondrosarcoma. Bone tumors with this classification are recommended to receive further evaluation with either short-term follow-up or a tissue biopsy. OT-RADS V is recommended for tumors that are highly suggestive of malignancy (≥50% probability of malignancy) and thereby should receive further evaluation with immediate tissue diagnosis. Representative lesions that would fall under this category include osteosarcoma, Ewing sarcoma, bone lymphoma, multiple myeloma, and metastasis. Lastly, OT-RADS VI is used to characterize known, biopsy-proven malignancies or recurrent lesions in the tumor bed prior to definitive therapy.
To determine the reliability and usefulness of the OT-RADS system, a multireader, retrospective, cross-sectional validation study was performed. In this study, 4 experienced MSK radiologists were presented with a sample set of 136 osseous tumors, 77 benign and 59 malignant, to grade after an initial training with the OT-RADS categories. The system was found to have an excellent reciever operating curve (ROC) (area under curve [AUC] = 0.92–0.97) and high interreader agreement (intraclass correlation coefficient [ICC] = 0.78). OT-RADS also showed high sensitivity (93%–100%) with moderate specificity (71%–86%), reflecting high diagnostic accuracy when differentiating between benign (OT-RADS I–III) and malignant lesions (OT-RADS IV–VI) compared to qualitative final diagnoses that are more traditionally seen on imaging reports. A follow-up study by Guirguis and colleagues was conducted to determine the impact of DWI sequences on the performance of OT-RADS. Although the reader confidence was higher using DWI with conventional imaging, the average ROC with DWI (AUC = 0.88–1.00) was determined to be statistically like that of conventional MR imaging, suggesting that conventional MR imaging sequences are sufficient for using OT-RADS to reliably and accurately characterize bone lesions.
OT-RADS provides a set of clearly defined, easy to apply categories for characterizing osseous lesions on MR imaging and functional imaging like DWI with practical recommendations that can aid in clinical management. One of the strengths of the system includes the utilization of a consistent, standardized lexicon and scoring system based on the WHO classification for bone tumors, thereby reducing the errors that may be associated with variable interpretation of the terminology used to describe the lesions. The validity and reliability of the system is also supported by 2 cross-sectional validity studies. Some of the limitations of the system include the lack of multicenter studies and prospective studies to determine the performance of the system in clinical practice. Additionally, these studies would benefit from the inclusion of readers across various experience levels as some radiologists with less experience in MSK radiology may not be as familiar with the classic presentations of bone lesions that are described in the OT-RADS lexicon.
Solitary Bone Tumor Imaging Reporting and Data System
The BTI-RADS categories were proposed in 2021 by Ribeiro and colleagues based on a study that evaluated imaging findings on CT and contrast-enhanced MR imaging that were more frequently associated with benign versus aggressive or malignant lesions. Three radiologists (2 MSK and 1 general) evaluated for the presence or absence of several imaging features on either CT or MR imaging, such as lesion size, tumor margins, periosteal reaction types, and so forth, on set of 230 solitary bone tumors (155 benign and 75 malignant tumors). The frequency of benign versus malignant lesions was then calculated for each imaging feature assessed to help classify the features as benign indicators, malignant indicators, or indeterminate features. Seven benign and 9 malignant indicators (6 minor and 3 major) were identified to be relevant in differentiating benign and malignant tumors. Indicators on MR imaging (lesion size, shape, no contrast enhancement, and presence or absence of soft tissue invasion), CT (transverse bone location, modified Lodwick–Madewell grades for tumor margins, aggressive periosteal reaction, and metastatic disease), and 3 general indicators (pelvic location, extremity location, age ≥50 years) were used. All 3 major malignant indicators (modified Lodwick–Madewell grade III tumor margins, aggressive periosteal reaction and suspected metastatic disease) were identified on CT and found to be associated with a malignancy frequency of over 80%.
Consequently, the authors proposed 4 BTI-RADS categories with increasing frequency of malignancy: BTI-RADS I through IV. BTI-RADS I describe benign lesions that have features of “do not touch” tumors with 2 or greater benign indicators and 1 or less minor malignant indicator. “Do not touch” bone lesions were considered by the authors to be geode (subchondral cyst and synovial herniation pit), subperiosteal hematoma, fibrous cortical defect and nonossifying fibroma, enostosis, simple bone cyst, and bone infarction. BTI-RADS II lesions are likely benign lesions that lack features of the typical “do not touch” lesions and include 2 or greater benign indicators and 1 or less minor malignant indicator. BTI-RADS III lesions are suspicious for malignancy and present on CT and MR imaging with 1 or less benign indicator or less than 3 minor malignant indicators. Lastly, BTI-RADS IV lesions are likely malignant and include 3 or greater minor malignant indicators or any major malignant indicator.
BTI-RADS provides a structured report for analyzing solitary bone lesions with associated recommendations like suggestions for the timing of appropriate referrals to oncology centers for further management. However, BTI-RADS relies on patients receiving both CT and MR imaging to grade bone lesions, which can be challenging for patients from both financial and logistic standpoints. , Additionally, as with many of the other systems currently available, BTI-RADs is reliant on expert opinion and lacks external evaluation.
Recently, a study by Lemore and colleagues aimed to address some of these major shortcomings by proposing a BTI-RADS 2.0 for further risk stratification based on a machine learning-based approach. BTI-RADS 2.0 proposed 4 risk classes based on model predictions and probability thresholds corresponding to different malignancy frequencies: BTI-RADS II—definitely benign; BTI-RADS III—probably benign; BTI-RADS IV—suspicious for malignancy; and BTI-RADS V—highly suggestive of malignancy like OT-RADS approach. The authors also sought to objectively identify the most relevant characterization features and found that the highest-ranked features for discriminating between benign and malignant solitary bone lesions were Lodwick–Madewell grade III tumor margins (CT feature), aggressive periosteal reaction (CT feature), and irregular shape (general feature), with malignancy rates ranging from 77% to 90%. Using a multimodal approach that encompassed 27 characterization features, the machine-based learning approach achieved an accuracy, sensitivity, and specificity of 81%, 87%, and 75%, respectively, performing slightly inferior to expert radiologists. While lacking data evaluating the clinical utility of BTI-RADS 2.0, this marks an interesting approach that offers a more objective method of establishing relevant criteria to be included in RADS guidelines without overreliance on potentially subjective expert opinions.
Related posts:
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 Wrist Ligaments Injuries and Instability
Wrist Ligaments Injuries and Instability
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


