Lower extremity peripheral nerve injuries leading to sensorimotor disturbances can significantly impede athletic performance and return to play. Electrodiagnostic studies are limited by operator dependency, limited sensitivity in the acute phase, and sometimes inability to localize a lesion, particularly if only partial (ie, fascicular) or multifocal injury is present. This article highlights the clinical value of MR neurography in diagnosing and managing sports-related peripheral nerve injuries, including iatrogenic nerve-related complications following sports surgeries.
Key points
-
•
Lower limb peripheral nerve injuries in athletes are relatively uncommon and may be underrecognized, leading to persistent deficits if not diagnosed early and managed appropriately.
-
•
MR neurography (MRN) enables precise localization of a nerve injury and can simultaneously assess the involved nerve and regional musculature for denervation.
-
•
MRN may demonstrate an aberrant nerve course and loss of fascicular architecture, suggesting scar tethering and neuroma formation, respectively, that may require surgical intervention.
Abbreviations
| 2D | 2-dimensional |
| 3D | 3-dimensional |
| CPN | common peroneal nerve |
| DESS | double-echo steady-state |
| EDX | electrodiagnostic testing |
| FSE | fast spin echo |
| FOV | field-of-view |
| LFCN | lateral femoral cutaneous nerve |
| MRN | MR neurography |
| PD | proton density |
| PDw | proton density weighted |
| PSIF | time reversed fast imaging with steady-state precession |
| SNR | signal-to-noise ratio |
| STIR | short-tau inversion recovery |
| T | Tesla |
Introduction
Sports-related activities account for approximately 6% of all peripheral nerve injuries. Although less common than upper limb injuries, lower extremity nerve injuries may be overlooked, particularly when associated with concurrent ligamentous, muscular, or osseous trauma. Diagnosis can be challenging due to the potential for multifocal involvement and partial injury, where only some of the fascicular bundles of the entire cross-sectional area of a nerve may be disrupted. Additionally, surgical management of primary lower extremity injuries may itself lead to iatrogenic nerve injury. Electrodiagnostic testing (EDX) is sometimes helpful to determine the site and severity of a nerve injury, but it is operator-dependent, and may be inconclusive or nonrevealing in the acute phase (ie, first weeks) when insufficient time has elapsed for muscle denervation to ensue. ,
MR neurography (MRN) serves as an important adjunct to EDX for evaluation of peripheral neuropathies. MRN provides high-resolution anatomic detail of peripheral nerves, enhancing diagnostic accuracy and assisting in surgical planning. , Recent advancements in MR hardware and software now facilitate higher spatial resolution to be obtained, to provide improved assessment of small-caliber nerves that may otherwise not be reliably identified. Furthermore, MRN allows for comprehensive evaluation of both nerves and regional musculature, providing insights into the presence and chronicity of denervation.
This article outlines key technical considerations for lower extremity MRN, summarizes common sports-related nerve injuries from the pelvis to the foot, and highlights MRN’s role in detecting iatrogenic nerve injuries following surgery for non-neurologic sports injuries.
MR neurography techniques and anatomic correlates
General Technical Considerations
If clinical and/or EDX studies cannot precisely localize a lesion, it is recommended to initially focus imaging at the most symptomatic site or the area of previous injury or surgery. Skin markers should be placed over palpable abnormalities and/or surgical scars, when present, to assist in anatomic localization. When feasible, real-time supervision by an experienced MRN radiologist facilitates protocol adjustments and coil repositioning to maximize the diagnostic yield.
MRN is ideally performed at 3.0 Tesla (T) due to its superior gradient performance and nearly double signal-to-noise ratio (SNR) compared to 1.5 T. To optimize SNR and spatial resolution, use of a flexible phased-array surface coil that closely conforms to anatomic contours is preferred, as this reduces the distance between the coil elements and the region of interest. MRN relies on heavily T2-weighted (T2w), fat-suppressed sequences—both 2-dimensional (2D) and 3-dimensional (3D)—which typically provide the necessary contrast to delineate the nerve from background tissues and sufficient fluid-sensitivity to maximize sensitivity to nerve pathology. Such 2D sequences provide high in-plane resolution (typically 0.3–0.5 mm), and when acquired orthogonal to the longitudinal course of the nerve, facilitate detailed assessment of the nerve’s fascicular architecture. 3D MRN commonly includes either fat-suppressed fast spin echo (FSE) (including motion-sensitive driven-equilibrium based techniques such as 3D CRANI ), or steady-state free-precession based sequences, such as time-reversed fast imaging with steady-state precession (PSIF) and double-echo steady-state (DESS) sequences. When acquired isotropically, 3D MRN is particularly effective for long-axis visualization of peripheral nerves to detect subtle morphologic changes and deviations in their course. An MRN examination also typically includes either a 2D proton-density weighted (PDw) FSE sequence for anatomic delineation, acquired axially and sometimes with additional planes to provide higher in-plane resolution imaging than T2w sequences for evaluating the surrounding anatomy and fascicular architecture.
Recommended MRN protocols for the lumbosacral plexus and lower extremity are summarized in Tables 1 and 2 , respectively. , Optionally, intravenous gadolinium administration can facilitate vascular signal suppression, improving the visualization of small nerve branches that may be obscured by adjacent isointense vessels. Susceptibility artifacts from metallic hardware can be mitigated using multispectral metal artifact reduction techniques, such as multiple-acquisition variable-resonance image combination (MAVRIC, GE HealthCare, Waukesha, WI) and slice encoding for metal artifact correction (SEMAC, Siemens Healthineers, Erlangen, Germany). However, these are often associated with trade-offs in reduced in-plane spatial resolution or increased scan time. In some cases, severe susceptibility artifact may necessitate imaging at 1.5 T rather than 3T, when the nerves of interest are near the hardware.
Table 1
Recommended 3.0 T lumbosacral plexus MR neurography protocol
| Sequence Types | |||||
|---|---|---|---|---|---|
| Parameters | 2-Dimensional Proton Density Weighted-Fast Spin Echo | 2-Dimensional T2-Weighted Fast Spin Echo | Oblique 2-dimensional T2-Weighted-Fast Spin Echo | 3-Dimensional Double-Echo Steady-State | 3-Dimensional Short Tau Inversion Recovery-Fast Spin Echo |
| Imaging plane(s) | axial | axial or coronal | oblique sagittal | coronal or oblique coronal | |
| TR/TE/TI (ms) | 3500–6000/30/- | 3500–6000/85/- | 3500–6000/85/- | 14.7/5.1–9.7/- | 3300 /80/250 |
| FOV (cm) | 29–32 | 29–32 | 20 | 30–32 | 30–32 |
| Matrix size | 512 × 320 | 320 × 192 | 320 × 192 | 356 × 356 | 288 × 288 |
| Slice thickness/gap (mm) | 4.5/0.0 |
4.5/0.0 (axial)
3.0/0.0 (coronal) |
2.5/0.0 | 0.9/0.0 | 1.2/0.0 |
| Echo train length | 10 | 15 | 17 | 2 | 130 |
| Bandwidth (Hz/pixel) | 195 |
391 (axial)
521 (coronal) |
521 | 234 | 347 |
| Fat suppression technique | – | Dixon | Dixon | water-excitation | STIR |
| Parallel imaging factor | 1.75 | 1–1.5 | 1–1.5 | 2 × 1–1.5 | 1.5 × 1 |
| Scan time (min) | 3–5 | 4–6 | 6–8 | 5–6 | 5–6 |
Abbreviations: TE, echo time; TI, inversion time; TR, repetition time.
Table 2
Recommended 3.0 T lower extremity MR neurography protocol
| Parameters | Sequence Types | ||
|---|---|---|---|
| 2-Dimensional Proton Density Weighted-Fast Spin Echo | 2-Dimensional T2-Weighted-Fast Spin Echo | 3-Dimensional Double-Echo Steady-State | |
| Imaging plane(s) | axial | axial | axial |
| TR/TE (ms) | 3500–6000/30 | 3500–6000/85 | 14.6/5.2, 9.4 |
| FOV (cm) | 8–18 | 10–20 | 10–20 |
| Matrix size | 512 × 352 | 320 × 224 | 320 × 320 |
| Slice thickness/gap (mm) | 2.5–3.5/0.0 | 2.5–3.0 | 1.6/0.0 |
| Echo train length | 10–15 | 12–16 | – |
| Bandwidth (Hz/pixel) | 325 | 244 | 162 |
| Fat suppression technique | – | Dixon | water-excitation |
| Parallel imaging factor | 1.75 | 1–1.5 | 1.5 × 1 |
| Scan time (min) | 3–5 | 4–6 | 4–6 |
Fig. 1 provides an illustrative overview of the key lower extremity nerves, their normal MRN appearances, and anatomic courses.
Overview of key lower extremity nerves: Normal MRN appearance and anatomic course.
Lumbosacral Plexus
The lumbosacral plexus (LSP) comprises the lumbar (T12–L4) and sacral (L4–S4) plexi and its anatomy has been comprehensively reviewed in a recent publication. The optimal coil configuration typically involves combining a posterior spine array coil with a flexible anterior surface array coil wrapped around the lumbar and pelvic regions. Coronal imaging usually uses a wide field-of-view (FOV) of 29 to 32 cm, spanning from the L3 superior endplate to the lesser trochanters. The small-caliber nerves arising from the L1 and L2 roots (iliohypogastric, ilioinguinal, and particularly genitofemoral nerves) may be difficult to reliably visualize on both steady-state free-precession sequences (due to motion) and short tau inversion recovery (STIR) FSE sequences (due to T2 blurring). For protocol efficiency, the anteroposterior scanning field can be tailored to the specific nerves of interest. For sciatic nerve imaging, posterior coverage should include the greater sciatic foramen to visualize the nerve as it exits the pelvis. In contrast, assessing the femoral and lateral femoral cutaneous nerves requires inclusion of the subcutaneous fat anterior to the anterosuperior iliac spine to fully capture their course along the anterior pelvis and thigh. For a targeted assessment, an oblique-sagittal T2w Dixon scan with a smaller FOV (∼20 cm)—plotted orthogonally to the nerve—enhances visualization of fascicular architecture.
Thigh to Lower Leg
A high-density flexible surface coil, typically 16 to 23 channels, is essential for optimizing SNR and maintaining high spatial resolution across multiple stations in the thigh and lower leg. This is preferred over a combination of several flexible coils that typically results in poorer conformity to the skin and reduced density of elements covering a particular region, thereby resulting in lower SNR. Key nerves relevant to MRN of the thigh and lower leg include the sciatic nerve and its branches—the tibial and common peroneal nerves—as well as the sural and saphenous nerves.
Ankle to Foot
To image the ankle and foot nerves, a dedicated ankle coil or multipurpose high-density flexible array can be used; the tradeoff of the latter option is that the ankle cannot be placed in full dorsiflexion to obtain standard anatomic imaging planes. For small-caliber lower extremity nerves, such as the saphenous and deep peroneal—where interpretation may be hindered by adjacent vessels of similar size and signal intensity—the inclusion of fat-suppressed 3D gradient-echo techniques (eg, PSIF and DESS) are especially helpful as they provide simultaneous vascular suppression, high through-plane spatial resolution, and when acquired isotropically, or nearly isotropically, afford the ability to create multiplanar reconstructions to evaluate the nerve’s course in multiple arbitrary planes.
Advanced Techniques and Future Directions
Deep learning-based reconstruction methods have been shown to enhance nerve conspicuity, and have made traditionally time-consuming 3D high-resolution imaging more clinically feasible. Bone-sensitive MR imaging sequences, such as gradient-echo or zero echo time imaging, are valuable for assessing adjacent osseous structures—particularly when CT has not been performed—by aiding in fracture assessment or preexisting osseous anomalies, such as osteochondromas, in relation to regional nerves ,
While not routinely used in practice, quantitative T2 mapping shows promise in assessing active muscle denervation, correlating with motor unit recruitment loss observed on EMG. Recent sequence innovations have enabled simultaneous qualitative assessment and quantitative T2 mapping, providing image quality comparable to conventional T2w imaging while facilitating the detection of abnormal T2 values in nerves and muscles, as demonstrated in patients with foot drop. Additionally, T1w Dixon-based fat quantification can be used to assess fat infiltration in chronically denervated muscles.
Regional overview of common sports-related lower extremity nerve injuries
Lumbosacral Plexus to Thigh
Lumbosacral plexus
Low back pain is a common issue among athletes, with more than 30% experiencing such episodes during their careers. Repetitive torsion, flexion, extension, and axial loading place considerable stress on the lumbar spine, predisposing athletes to disc herniation, which was identified in 58% of MR scans among Olympic athletes with low back pain. Lumbosacral plexus (LSP) MRN not only localizes radiculopathy but also offers superior symptom correlation compared to conventional spine MR imaging, influencing patient management and contributing to improved clinical outcomes.
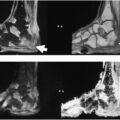
Sacral stress fractures are an underrecognized cause of low back and buttock pain in athletes. While most cases result from repetitive loading during high-endurance activities such as long-distance running and high-impact aerobic exercise, insufficiency fractures may also occur, particularly in athletes exhibiting features of the Female Athlete Triad—disordered eating, menstrual dysfunction, and low bone mineral density. Equestrian sports, which carry a high risk of falls from height, further increase vulnerability to sacral injury. Notably, insufficiency fractures can induce exuberant bone formation that impinges upon adjacent nerve structures, including the L5 and S1 nerve roots and the lumbosacral trunk. In such cases, LSP MRN facilitates the precise localization of nerve impingement ( Fig. 2 ). In addition, MRN is valuable for evaluating associated nerve stretch injuries and more severe forms, such as preganglionic avulsion injuries, which may occur in high-energy trauma scenarios such as motor vehicle collisions ( Table 3 ).
58-year-old female with right-sided low back pain and sciatica for 1 month following a fall while jogging. Axial PDw ( A ) and T2w Dixon ( B ) images demonstrate fracture of the right hemisacrum with prominent marrow edema. Periosteal new bone formation (orange arrows ) along the anterosuperior aspect of the right sacral ala impinges on the extraforaminal right L5 nerve root (blue arrow ), which is mildly hyperintense.
Table 3
Lower extremity nerve injuries mechanisms and MRN findings by region and nerve
| General Anatomic Region | Involved Peripheral Nerve Segment | Common Sports/Iatrogenic Mechanisms | Injury Site(s) | MRN Findings |
|---|---|---|---|---|
| Pelvis/proximal to midthigh | Nerve root | Disc herniation from repetitive axial loading (eg, weightlifting and gymnastics) | Spinal canal and neuroforamen | Herniated disc compressing nerve root with nerve T2w hyperintensity and enlargement |
| L5–S1 roots and lumbosacral trunk | Sacral repetitive stress fracture (long-distance running); traumatic sacral fracture (equestrian fall) | Near sacral ala or anterior sacrum | Nerve T2w hyperintensity and enlargement; adjacent bone marrow edema or callus formation | |
| Sciatic | Proximal hamstring tear; surgical hamstring repair | Near ischial tuberosity | Nerve T2w hyperintensity, perineural scarring, and nerve tethering | |
| Sciatic | Deep gluteal syndrome; repetitive hip abduction/extension (eg, martial arts and runners) | Piriformis, obturator internus, and ischiofemoral space | Nerve T2w hyperintensity and enlargement | |
| Femoral | Hyperextension injury or iliacus hematoma (eg, skiing and gymnastics) | Iliopsoas compartment to femoral triangle | Nerve T2w hyperintensity and enlargement; may show adjacent hematoma compressing nerve | |
| Lateral femoral cutaneous | Compression from tight garments/equipment; hip arthroscopy | Anterior to anterior superior iliac spine | Nerve T2w hyperintensity and enlargement | |
| Pudendal | Prolonged perineal pressure (eg, cycling); surgical trauma | Alcock’s canal | Asymmetric obliteration of perineural fat plane; nerve T2w hyperintensity and enlargement occasionally seen | |
| Distal thigh, knee, and lower leg | Sciatic | Popliteal nerve block | Injection site | Long-segment T2w hyperintensity along sciatic nerve |
| Common peroneal | Knee dislocation (eg, football and skiing); fibular head trauma; meniscal repair | Fibular neck | Nerve T2w hyperintensity and enlargement, neuroma-in-continuity, or nerve discontinuity | |
| Superficial/deep peroneal | Compartment syndrome (acute or exertional); fasciotomy | Anterolateral leg | Muscle edema (post-exercise if exertional) | |
| Saphenous | Posterolateral knee instability; pes anserine bursitis; knee arthroscopy | Adductor canal; medial or lateral knee | Nerve T2w hyperintensity and enlargement, neuroma-in-continuity, or nerve discontinuity | |
| Tibial | Iatrogenic injury during tibial fixation (instrument overshoot) | Fracture site/surgical corridor | Nerve T2w hyperintensity and enlargement, discontinuity, and perineural fibrosis | |
| Foot | Tibial (medial/lateral plantar) | Tarsal tunnel syndrome; tarsal tunnel release | Tarsal tunnel | Nerve T2w hyperintensity and enlargement; mass effect (eg, ganglion) |
| Plantar (medial/lateral) | Overpronation, repetitive strain (Baxter’s neuropathy and jogger’s foot) | Medial heel, knot of Henry | Nerve T2w hyperintensity and denervation in foot muscles | |
| Digital | Morton’s neuroma (eg, tight shoes and running) and Joplin neuroma (eg, bunion surgery) | Along plantar great toe or between metatarsals | Perineural nodular thickening with intermediate to low T2w signal |
Sciatic nerve
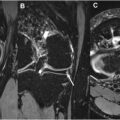
The sciatic nerve is particularly vulnerable to injury following hamstring tears—both acutely from hemorrhage and edema, and chronically from scarring, mass effect, or tethering due to the close proximity of these structures. MRN findings of complete conjoined tendon avulsion, greater tendon retraction, sciatic nerve T2w hyperintensity, and circumferential perineural hematoma are also associated with increased difficulty of sciatic nerve dissection intraoperatively ( Fig. 3 ). Similarly, MRN may reveal extensive perineural scarring and sciatic nerve tethering to the repaired hamstring tendon in patients presenting with new-onset sciatica after proximal hamstring tendon repair.
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 High-Resolution Imaging of Knee Meniscus Anatomy and Tears
High-Resolution Imaging of Knee Meniscus Anatomy and Tears
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


