Accurate detection and characterization of meniscal tears is essential for managing symptomatic knees. Conventional two-dimensional (2D) magnetic resonance imaging imaging (MR) has served as the standard for this purpose; however, recent advances in three-dimensional (3D) isotropic MR imaging offer improved spatial resolution and multiplanar reformation capabilities that enhance diagnostic accuracy. High-resolution 3D MR sequences complement and, in select scenarios, surpass 2D MR sequences in delineating complex meniscal patho-anatomy. This article reviews normal anatomy, meniscal tear types, MR imaging criteria for tear, and imaging correlates of common lesions with emphasis on the advantages, limitations, as well as diagnostics performance of routine 2D and volumetric 3D sequences.
Key points
-
•
Two-dimensional (2D) magnetic resonance (MR) imaging remains the most commonly used method for meniscal imaging because of its wide availability, fast acquisition, and high in-plane resolution.
-
•
Three-dimensional (2D) isotropic volumetric MR imaging sequences provide thin-slice imaging without interslice gap and multiplanar reformation capabilities, enhancing detection of complex, radial, and root tears.
-
•
3D MR imaging can improve preoperative planning and postoperative assessment, especially in evaluating meniscal tear morphology.
-
•
Diagnostic performance of 3D MR imaging is comparable to or better than 2D MR imaging in several studies, with improved reader confidence and reproducibility.
Abbreviations
| 2D | 2-dimensional |
| 3D | 3-dimensional |
| ACL | anterior cruciate ligament |
| FS | fat suppression |
| LMORT | lateral meniscus oblique radial tear |
| MPR | multiplanar reformation |
| MR | magnetic resonance |
| PCL | posterior collateral ligament |
| PD | proton density–weighted |
| PHLM | posterior horn of the lateral meniscus |
| SNR | signal-to-noise ratio |
| SPACE | Sampling Perfection with Application-optimized Contrasts using different flip angle Evolutions |
| T2-weighted | T2-weighted |
Introduction
Meniscal injuries are highly prevalent in athletic and aging populations, contributing significantly to musculoskeletal morbidity. In sports, they account for approximately 15% to 20% of all knee injuries, particularly in athletes engaged in pivoting and high-impact activities, with traumatic tears frequently occurring alongside anterior cruciate ligament (ACL) injuries in up to 70% of cases. In older adults, degenerative meniscal tears are common, affecting up to 60% of individuals over age 50—even in asymptomatic cases—and are strongly associated with early osteoarthritis progression. ,, These injuries are a major driver of knee magnetic resonance (MR) imaging utilization and arthroscopic procedures globally. Left untreated, meniscal damage can accelerate cartilage degeneration and lead to long-term joint dysfunction and disability. , MR imaging, the modality of choice for noninvasive evaluation of the knee menisci, allows for detailed assessment of meniscal morphology, tear patterns, anatomic zonal location, as well extent of a tear, and associated intra-articular pathology, providing critical information for diagnosis, treatment planning, and postoperative monitoring. ,, MR imaging can distinguish between traumatic and degenerative tears, classify tear types (eg, horizontal, longitudinal-vertical, radial, complex), and evaluate tear extent in all planes. It also enables detection of indirect signs of injury such as parameniscal cysts, meniscal extrusion, and associated menisco-osteochondral unit dysfunction, cartilage or ligament damage. ,,
Conventional 2-dimensional (2D) MR imaging sequences, for example, proton density–weighted (PD) or T2-weighted (T2) MR imaging with or without fat suppression (FS), reliably detect meniscal tears, with reported sensitivities and specificities exceeding 80% to 90% compared to arthroscopy, the reference standard. ,,,,, Traditional 2D MR imaging, using PD and T2 sequences acquired in sagittal, coronal, and axial planes, typically employs 3 to 4 mm slice thickness with interslice gaps, which can result in partial volume averaging and limited visualization of obliquely oriented or small tears. Despite its high in-plane resolution and widespread availability, 2D MR imaging lacks multiplanar reformation capabilities and may miss subtle or complex meniscal injuries. As such, the evaluation of meniscal pathology by MR imaging has evolved from conventional 2D imaging to advanced 3-dimensional (3D) isotropic techniques, with similar to slightly superior diagnostic performance for the detection of subtle meniscal tears. Advanced 3D isotropic MR imaging techniques (eg, SPACE, CUBE, VISTA) generate thin-slice (typically 0.5–0.7 mm), high-resolution images with multiplanar reformation capabilities, improving visualization of subtle, complex, or root tears. ,,,,,,,, Although slightly more susceptible to motion artifacts and sometimes longer in acquisition, 3D MR imaging has demonstrated comparable or superior sensitivity and specificity to 2D imaging in detecting meniscal tears, particularly when assessing subtle or nonorthogonal lesions. , The purpose of this article is to discuss normal meniscal anatomy and pathology on MR imaging, highlighting the various advantages and limitations of conventional 2D and advanced 3D sequences in routine clinical practice.
Normal meniscus anatomy on magnetic resonance imaging
The knee contains 2 menisci—medial and lateral—each serving as a fibrocartilaginous cushion between the femoral condyles and tibial plateau. The medial meniscus is C-shaped, broader posteriorly, and more tightly anchored to the joint capsule and medial collateral ligament, making it more prone to injury ( Fig. 1 ). The lateral meniscus, by contrast, is more circular and mobile, with looser capsular attachments and stabilization by means of the meniscofemoral ligaments ( Fig. 2 ). Meniscal vascularity is regionally divided into 3 zones: the red-red zone (outer third) is well vascularized; the red-white zone (middle third) has limited perfusion, and the white-white zone (inner third) is avascular. , These zones have important implications for healing potential and surgical decision making, as tears in vascular regions are more amenable to repair. On a microscopic level, the menisci are composed predominantly of type 1 collagen fibers, organized primarily in a circumferential orientation, with radial tie fibers providing shear resistance and structural coherence. This architecture supports the transmission and distribution of axial loads into hoop stresses. The vascularity pattern, which diminishes centrally, is critical for tissue regeneration following injury. Histologically, the outer vascular zone contains more fibroblastic cells and vascular elements, whereas the inner region consists of sparsely cellular, fibrocartilaginous tissue embedded in a dense extracellular matrix. ,
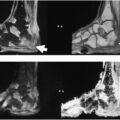
Normal medial meniscus on 3D MR imaging. ( A ) Axial multiplanar reformation (MPR) derived from sagittal 3D T2-FS, ( B and C ) sequential sagittal 3D T2-FS, ( D – F ) sequential coronal MPR derived from 3D T2-FS depict a normal C-shaped medial meniscus ( white arrow ) tightly adherent to the joint capsule and medial collateral ligament.
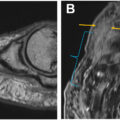
Normal lateral meniscus on 3D MR imaging. ( A ) Axial MPR derived from sagittal 3D T2-FS, ( B and C ) sequential sagittal 3D T2-FS, ( D – F ) sequential coronal MPR derived from 3D T2-FS depicts a normal lateral meniscus ( white arrow ). Note the relationship of the popliteal tendon ( asterisk ) hiatus relative to the meniscus midbody and posterior horns.
MR imaging provides excellent visualization of normal meniscal anatomy and its zonal architecture. On 2D MR imaging, the menisci appear as low-signal, triangular structures in the sagittal plane, with the body of the meniscus typically visible as a bowtie-shaped signal on 2 or more consecutive slices. , Coronal images help evaluate meniscal height and extrusion, while axial images offer detailed assessment of root attachments. However, the limited slice orientation and nonisotropic resolution of 2D MR imaging can obscure subtle or complex anatomy. In contrast, 3D isotropic sequences allow for high-resolution multiplanar reformatting, improving delineation of root attachments, interhorn continuity, and radial fiber orientation. , These features are particularly valuable in assessing root tears, anatomic variants, and subtle morphologic abnormalities that may be challenging to detect on conventional 2D knee MR imaging sequences because of differences in slice thickness and interslice gaps. ,
Magnetic resonance imaging techniques for meniscus imaging
Conventional 2D MR imaging sequences remain the cornerstone of routine knee imaging and provide reliable assessment of meniscal morphology and pathology. Commonly used sequences include PD and T2-weighted MR imaging with and without fat suppression acquired in multiple orthogonal planes—sagittal, coronal, and axial. These sequences typically use 3 to 4 mm slice thickness with 0.5 to 1 mm interslice gaps, which can result in partial volume averaging and occasional signal dropout at the meniscal margins. Despite these limitations, optimized 2D sequences offer high in-plane resolution and remain widely available on most clinical MR imaging systems. ,,,,
Advanced 3D MR imaging sequences have emerged to overcome the spatial limitations of 2D imaging by acquiring thin-slice isotropic datasets that can be reformatted into any desired plane. Key vendor-specific sequences include SPACE (Sampling Perfection with Application-optimized Contrasts using different flip angle Evolutions, Siemens, Erlangen, Germany), CUBE (General Electric (GE) Healthcare— Waukesha, Wisconsin, USA), and VISTA (Philips— Best, The Netherlands). These fast spin-echo–based 3D sequences achieve slice thicknesses of 0.5 to 0.7 mm with isotropic resolution, reducing interslice gaps and enhancing anatomic detail. Improvements in parallel imaging, variable flip angle techniques, and compressed sensing have reduced acquisition times while maintaining excellent signal-to-noise ratio (SNR) and tissue contrast, making them increasingly viable for routine use. ,,,,,,
Meniscal tear classification and magnetic resonance imaging appearance
Tear Types and Morphologies
Meniscal tears exhibit a wide range of morphologies that influence treatment decisions and prognosis; they are categorized by their shape and location when visualized on MR imaging, in which high-intensity intrameniscal signals against otherwise low-intensity meniscal tissue communicate with at least 1 articular surface on 2 consecutive 2D or 3D knee MR imaging sequences. , Common tear types include longitudinal-vertical, horizontal, radial, flap, complex, and root tears, and accurate characterization and description on MR imaging is critical for treatment planning. Table 1 describes the various meniscal types, MR imaging appearance, common location, and clinical significance of each tear type.
Table 1
Common meniscal tear types, definition, magnetic resonance imaging appearance, common location, and clinical significance
| Tear Type | Definition | Typical MR imaging Appearance | Common Location | Clinical Significance |
|---|---|---|---|---|
| Longitudinal tear | Vertical tear parallel to the long axis of the meniscus, perpendicular to the tibial plateau | Vertical linear signal extending to superior/inferior surface, divides the meniscus into central and peripheral components, may displace if large | Posterior horn of medial meniscus | Maybe amenable to repair in vascular zones |
| Horizontal tear | Splitting of meniscus parallel to tibial plateau | Horizontal linear signal dividing the superior and inferior surfaces; parallel to the tibial plateau; contacts articular surface or free edge centrally | Posterior horn and body | Common in degenerative disease; associated with parameniscal cysts |
| Radial tear | Perpendicular to circumferential fibers, extending from free edge | Ghost meniscus, truncation of meniscal body, radial cleft | Central third (white-white zone) | Disrupts hoop stress, may mimic total meniscectomy biomechanically |
| Flap (parrot-beak) tear | Oblique tear with a displaced meniscal fragment | Sharp, oblique linear signal; displaced flap fragment | Midbody of medial or lateral meniscus | May cause mechanical symptoms, often unstable |
| Complex tear | Combination of two or more tear patterns (eg, radial + horizontal) | Irregular morphology and signal intensity | Often in degenerative knees | Poor healing potential, often not suitable for repair |
| Bucket-handle tear | Longitudinal tear with central displacement of inner fragment | Double PCL sign; absent bowtie sign; displaced fragment in intercondylar notch | Posterior horn of medial meniscus | Often causes locking, requires urgent surgical attention |
| Root tear | Tear or avulsion at the meniscal root attachment | High signal at root insertion, ghost meniscus, radial tear-like morphology at attachment | Posterior horn root (medial > lateral) | Functionally similar to meniscectomy, associated with joint degeneration |
| Meniscocapsular separation (Ramp lesion) | Tear at the junction between meniscus and joint capsule | High signal line at meniscocapsular junction, fluid tracking into peripheral space | Posterior horn of medial meniscus | Associated with instability and ACL tears |
| Wrisberg rip | Longitudinal tear in periphery of lateral meniscus and capsule | Vertical line visible beyond 14 mm lateral to lateral margin of posterior cruciate ligament | Periphery of posterior horn of lateral meniscus | Associated with posterior instability and ACL tears |
| Lateral Meniscus Oblique Radial Tear | Radial or oblique tear through meniscus substance | Oblique radial tear | Lateral meniscus between popliteal hiatus to mid-body | Associated with loss of hoop tension and ACL tears as well as lateral collateral ligament complex injury |
Longitudinal tears
Longitudinal-vertical tears run perpendicular to the tibial plateau and parallel to the long axis of the meniscus, dividing the meniscus into central and peripheral halves. More commonly occurring in younger people after significant trauma to the knee, these tears typically present as a vertically oriented line of high signal intensity in contact with 1 or both articular surfaces on MR imaging. , Longitudinal tears tend to have a higher predilection for the peripheral third of the meniscus and posterior horns, which renders them more amenable to surgical repair given the richer vascularization of the afflicted area.
Horizontal tears
Horizontal or cleavage tears ( Fig. 3 ) run parallel to the tibial plateau through the midmeniscal body and, compared with longitudinal tears, are more commonly occurring in adults over 40 years with underlying degenerative changes and absent inciting event or trigger. A horizontally oriented line of high signal intensity in contact with either the meniscal surface or the free edge is characteristic on MR imaging, and, when completely extending to the periphery, tends to be associated with parameniscal cysts, likely because of direct communication with joint fluid. These tears are more prevalent in the white-white zone and usually chronic when diagnosed, thus less amenable to surgical repair, with the treatment often involving partial meniscectomy and open cystectomy with decompression of the associated parameniscal cyst when applicable. ,
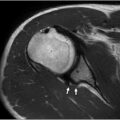
67-year-old woman with left knee pain. Coronal ( A ) MPR derived from sagittal ( B ) acquisition of 3D T2-FS of the left knee depicts a horizontal tear ( arrow ) of the medial meniscus midbody.
Radial tears
Radial tears originate from the free edge of the meniscus and run perpendicular to the tibial plateau and long axis of the meniscus, transecting the longitudinal collagen bundles in their course toward the periphery ( Fig. 4 ). Consequently, the meniscal hoop strength is significantly compromised, which results in a precipitous loss of function with possible meniscal extrusion. Similar to horizontal tears, radial tears more commonly occur in the white-white zone and are thus less amenable to surgical repair; however, MR imaging detection is often challenging, which can result in preoperative underdiagnosis. Radial tears have a higher predilection to either the posterior horn of the medial meniscus or the junction of the anterior horn and body of the lateral meniscus. , Various MR imaging findings have been identified with radial tears depending on the orientation of the injury relative to the imaging axis, including the truncated triangle sign, the cleft or marching cleft sign, and the ghost meniscus sign. On axial sequences, radial tears can present as clefts with perpendicular orientation to the meniscal free edge. Familiarity with these findings is critical to ensure optimal diagnostic performance during MR imaging evaluation and interpretation.
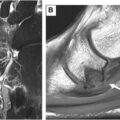
43-year-old man with left knee pain. Sagittal 3D T2-FS ( A ), coronal ( B ) and axial ( C ) MPR derived from 3D T2-FS MR imaging shows a small radial tear ( arrow ) at the lateral meniscus midbody.
Root tears
Root tears are radial-type tears with a high association with meniscal extrusion and, similar to radial tears, can face diagnostic challenges with MR imaging and arthroscopy, which subsequently impedes prompt evaluation and timely intervention. ,,,,,,,,, Coronal fluid-sensitive MR imaging g sequences allow for a better definition of the roots ( Fig. 5 ), which can in turn increase tear detection sensitivity and specificity. , Given their proximity to rich synovial blood that facilitates healing, acute root tears without significant associated degenerative changes are often promptly repaired.
64-year-old woman with left knee pain. Coronal ( A ) and axial ( B ) MPR derived from sagittal acquisition of 3D T2-FS of the left knee shows a complete radial tear ( arrow ) of the medial meniscus posterior root attachment. On the axial MPR ( B ), note perpendicular orientation of the fluid cleft relative to the free edge, compatible with a radial tear.
Complex and displaced tears
Complex tears amount to a combination of any 2 or all 3 longitudinal, horizontal, and radial tears, with an appearance characterized by meniscal fragmentation with multiplanar tear extension. On the other hand, displaced tears denote tears that involve either complete fragmentation of a piece of meniscus or flipping of a piece that otherwise remains attached to the rest of the meniscal body. Such tears include flap tears ( Figs. 6–8 ), which involve partially detached fragments of horizontal tears, bucket-handle tears, defined by complete longitudinal tears with centrally migrating fragments, and parrot-beak tears, which denote radial tears with partially detached fragments. Bucket-handle tears ( Fig. 9 ) are 7 times more likely to occur in the medial meniscus compared with the lateral meniscus and have various associated MR imaging findings that tend to confer higher sensitivity than specificity: an absent bow tie, a fragment within the intercondylar notch, a double posterior collateral ligament (PCL) ( Fig. 10 ), a double anterior horn or flipped meniscus, and a disproportionally small posterior horn. ,,,
65-year-old man with knee pain. Coronal 2D T2-FS ( A ) and PD ( B ) MR imaging of the left knee show a small complex flap tear of the medial meniscus midbody with small, displaced component in the meniscofemoral recess ( solid arrow ) and complete discoid lateral meniscus ( dashed arrow ).
50-year-old man with right knee pain. Coronal ( A ) and axial ( B ) MPR derived from 3D-acquired sagittal T2-FS of the right knee shows a complex flap tear in the medial meniscus midbody with displaced fragment ( arrow ) in the meniscotibial recess and flap component more conspicuous on the axial MPR. Note shiny corner sign or bone marrow in the medial tibial plateau ( asterisk ) indicative of menisco-osteochondral unit dysfunction.
52-year-old man with left knee pain. Sagittal 3D T2-FS ( A ) and 3D PD-FS ( B ) and axial oblique MPR derived from 3D T2-FS ( C ) depict a large displaced anterior horn and mid-body of the lateral meniscus into Hoffa fat pad ( arrow ).
56-year-old man with complex bucket handle tear of the medial meniscus. Axial oblique ( A ) and sagittal oblique ( B ) MPR derived from sagittal 3D T2-FS right knee MR imaging depicts a large displaced flap visible ( arrow ) in its entirety in the intercondylar notch.
40-year-old woman with left knee pain with prior anterior cruciate ligament reconstruction. Sequential sagittal MPR ( A and B ) derived from sagittal 3D T2-FS and 2D STIR ( C ) of the left knee demonstrate a complex bucket handle tear ( white arrow ) with double PCL sign. Note the normal PCL ( asterisk ).
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


