Shoulder impingement syndromes include subacromial, subcoracoid, and internal impingement. Impingement is primarily a clinical diagnosis. However, multimodality imaging is essential for defining anatomy and excluding differential considerations. Understanding the mechanisms of shoulder impingement and the ways each imaging modality aids diagnosis and treatment planning is of paramount importance. This article will describe the current understanding of shoulder impingement syndromes with an emphasis on subacromial impingement in describing state of the art imaging.
Key points
-
•
Shoulder impingement is a common cause of progressive shoulder pain.
-
•
The 3 described types of shoulder impingement are subacromial, subcoracoid, and internal impingement.
-
•
Shoulder impingement is primarily a clinical diagnosis, but multimodality imaging plays important roles in excluding differential considerations and devising optimal treatment strategies.
Abbreviations
| 2D | 2-dimensional |
| 3D | 3-dimensional |
| ACEA | acromiohumeral center edge angle |
| AP | anteroposterior |
| CSA | critical shoulder angle |
| CT | computed tomography |
| GIRD | glenohumeral internal rotation deficit |
| LAA | lateral acromial angle |
| LT | lesser tuberosity |
| MR | magnetic resonance |
| PD | proton density |
| SLAP | superior labral anterior posterior |
| SPGR | physeal-sensitive gradient recalled sequence |
| STIR | short inversion time inversion recovery |
| US | ultrasound |
| ZTE | zero echo time |
Introduction
Shoulder pain is the third most common musculoskeletal presentation in the primary care setting and the leading cause of atraumatic upper body pain. , Approximately half of patients have persistent shoulder pain and functional disability up to 3 years after initial presentation with nonoperative management. Shoulder impingement syndrome is the most common cause of progressive shoulder pain with an estimated 65% prevalence. This syndrome is characterized by insidious onset of pain, tenderness, and/or limited range of motion. Early diagnosis and treatment not only relieve pain and restore function but may also prevent progression of rotator cuff tendinopathy and tears.
Three distinct forms of shoulder impingement have been described. Subacromial impingement is the most common. Subcoracoid impingement, another type of external impingement, is relatively rare and may be underrecognized. Internal impingement, most commonly seen in repetitive and overhead throwing athletes, is a complex process with dynamic considerations in addition to osseous and soft tissue remodeling.
Subacromial impingement was first attributed to narrowing of coracoacromial arch by the coracoacromial ligament, anterior acromion, and subacromial spurs with cadaveric studies in 1972. Subacromial impingement was thought to occur due to intrinsic mechanical compression of the supraspinatus tendon and subacromial-subdeltoid bursa within this narrowed space, often exacerbated by overhead activities with shoulder abduction and flexion. However, the concept of subacromial impingement has since shifted from a purely mechanical model to a more complex multifactorial process involving multiple extrinsic factors. Common extrinsic etiologies are altered scapulothoracic and glenohumeral joint kinematics caused by thoracic hyperkyphosis and acromial or coracoacromial arch pathology. A form of secondary subacromial impingement may be attributable to instability in the throwing athlete. In either case, nonoperative management is preferred with acromioplasty and subacromial decompression often reserved for rotator cuff repair.
Subcoracoid impingement is the result of subscapularis tendon impingement between the coracoid process and the lesser tuberosity (LT) of the humerus. This often presents as anterior shoulder pain, exacerbated by forward flexion, adduction, and internal rotation. A decreased coracohumeral interval and increased coracoid overlap have been shown to be predictors for subcoracoid impingement. Nonoperative management is also preferred though coracoplasty may be performed to increase the coracohumeral interval and concurrent subacromial impingement should be simultaneously addressed. ,
Internal impingement was first described in its current form in 1992 and subsequently supported by cadaveric research. , This type of impingement primarily occurs in repetitive overhead throwing athletes, such as baseball pitchers and tennis players, and can also be seen in nonathletes but to a lesser degree of clinical significance. Internal impingement presents with pain most pronounced in the late cocking or early acceleration phase of throwing. A variety of dynamic and static forces contribute to the imbalance resulting in internal impingement. There is also overlap with several other syndromes including labral tears, rotator cuff tears, glenohumeral internal rotation deficit (GIRD), scapular dyskinesia, and instability. However, some findings that would be considered pathologic in the general population may be adaptive for the throwing athlete, and surgical repair to normal may limit the athlete’s ability to return to play.
Regardless of the etiology, shoulder impingement syndrome is primarily a clinical diagnosis with physical examination demonstrating up to 90% sensitivity, though specificity is lacking. , Therefore, imaging plays a critical role in excluding differential considerations and defining anatomic features that guide management. , Early intervention may prevent progression to debilitating outcomes secondary to natural history of disease. Imaging has been shown to enhance diagnostic accuracy, guide treatment decisions, and improve outcomes for patients with shoulder impingement syndrome. , This article aims to describe the developmental and degenerative mechanisms thought to contribute to shoulder impingement syndrome with a focus on the role of multimodality imaging.
Clinical diagnosis
A wide range of physical examination maneuvers are used in the evaluation of shoulder pain. Familiarity with the common physical examination findings associated with impingement can facilitate communication between radiologists and referring providers.
Subacromial Impingement
A positive Hawkins test elicits pain with maximal internal rotation of the shoulder at 90° of flexion with the elbow flexed. A positive test signals narrowing of the subacromial space between the greater tubercle and the coracoacromial ligament.
The Neer test is performed by stabilizing the scapula while passively elevating and internally rotating the arm. A positive test (Neer sign) elicits pain secondary to impingement between the greater tubercle and the acromial arch.
A positive Jobe test indicates supraspinatus pathology when downward pressure applied to the internally rotated arm positioned in 90° of abduction and 45° of forward flexion elicits pain or weakness. Painful arc is assessed during active abduction of the arm in the scapular plane. Pain between 60° and 120° indicates subacromial impingement.
Subcoracoid Impingement
Subcoracoid impingement presents as nonspecific and dull anterior shoulder pain with associated joint clicking exacerbated by forward flexion, adduction, and internal rotation. , Point tenderness of the coracoid process and maximal pain between 120° and 130° of forward flexion and internal rotation of the arm is highly indicative of subcoracoid impingement. The pain can also be referred to the upper arm and forearm.
Internal Impingement
Physical examination findings for internal impingement are often nonspecific. Tenderness along the posterior joint line is the most common sign with pain reproduced by positioning of the arm in 90° abduction and maximal external rotation in the throwing position. GIRD and internal impingement are thought to exist on a continuum of disabled thrower’s shoulder. Primarily seen earlier on in the overhead throwing athlete, GIRD is defined as a loss of internal rotation greater than the external rotation gain by at least 25° due to contracture of the posterior joint capsule. As the adaptive structural changes continue, internal impingement may occur because of a shift in the glenohumeral rotation point posteriorly and superiorly, which increases contact between the undersurface of the rotator cuff and the glenoid rim. Positive relocation test are commonly seen in clinical evaluation. , In particular, the O’Brien’s test uses active compression to evaluate for superior labral anterior posterior (SLAP) tears with positive test occurring with pain or clicking in the shoulder.
Subacromial impingement
Anatomic Variations and Degenerative Changes
Anatomic variations implicated in subacromial impingement include acromial shape, fusion anomalies, inferior osseous changes, and degenerative thickening of the coracoacromial ligament at its acromial attachment. ,
Acromial morphology is most commonly described as flat (Type 1), curved (Type 2), hooked (Type 3), and convex (Type 4). , Curved and hooked acromial morphologies are more often associated with rotator cuff pathology and respond more favorably to surgical intervention than conservative management. , However, the strength of this correlation is debated.
Subacromial spurs greater than 5 milimeters (mm) have also been associated with shoulder impingement and most commonly occur at the anteroinferior acromion. There also exist different types of spurs, such as traction, heel-type, bird beak, and medial spurs. , Traction spurs are formed from mechanical stress by the coracoacromial ligament or deltoid muscle within the subacromial arch. , The heel-type is most commonly associated with rotator cuff tears, specifically with bursal facing tears. ,
Alterations to coracoacromial ligament morphology may cause narrowing of the subacromial space contributing to impingement. Degeneration of the coracoacromial ligament, characterized by thinning of the ligament, may serve as a strong predictive factor for impingement syndrome and subsequent rotator cuff tear. , Coracoacromial ligament degeneration increases contact with the humeral head, initiating a progressive cycle that accelerates further coracoacromial ligament degeneration and worsens impingement. ,
An os acromiale, an unfused acromial ossification center seen in less than 10% of the population, is thought to be a risk factor for osseous shoulder impingement. The mesoacromion, the most common subtype, seems to be the most frequently associated with osseous impingement, though evidence remains inconclusive. , An os acromiale may develop inferior osteophytes at its synchondrosis or possibly predispose patients to early acromioclavicular arthritis. The distal acromion does not normally fuse until early adulthood, so this diagnosis should not be made before the age of 25 years.
Imaging Techniques and Findings
Imaging the painful shoulder in the setting of suspected subacromial impingement is usually a multimodality evaluation. Radiography, ultrasound (US), and magnetic resonance (MR) imaging are routinely employed. Radiographs are generally recommended as the first step. Further evaluation of the soft tissues may be obtained with US and/or MR imaging. Computed tomography (CT) is often reserved for preoperative planning. The strengths and limitations of each modality can be considered by understanding their inherent differences in spatial, contrast, and temporal resolution. Ultimately, shoulder impingement is a clinical diagnosis that may or may not be supported by imaging findings. It is important to recognize that there is a high prevalence of incidental findings, which has been shown to be as high as 96% in asymptomatic men between 40 and 70 years of age.
Radiographs
Radiography enables rapid image acquisition and is generally well-tolerated by patients with respect to required positioning. Although ionizing radiation is employed, the absorbed dose is very small. As shoulder radiographs have poor soft tissue contrast resolution, they may appear normal even in the setting of advanced impingement. ,, Although acromial morphology and subacromial spurs may be evident, the main utility of radiographic evaluation is to exclude differential considerations (ie, glenohumeral osteoarthritis, calcific tendinitis, osseous deformity, and so on).
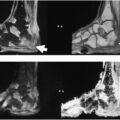
A radiographic series of the shoulder should contain at least 3 views. We commonly obtain neutral oblique anteroposterior (AP), outlet, and transaxillary views ( Figs. 1 and 2 ). The Grashey AP and transaxillary views are sufficient for excluding osteoarthritis, fracture, measurement of the acromiohumeral distance, and assessing for os acromiale. The outlet view allows for assessment of the acromioclavicular joint as well as the coracoacromial arch and subacromial spur morphology. Additional views, such as internal/external rotation views, may be requested but are not essential.
Routine radiographic evaluation of the right shoulder in a 65-year-old male with ( A ) neutral Grashey AP, ( B ) transaxillary, and ( C ) outlet views. The acromiohumeral interval is demarcated with brackets ( A , C ). The outlet view demonstrates a hooked, or Type 3, acromion with a decreased acromiohumeral interval far anteriorly ( A ). The acromion index is defined as distance of the lateral acromion from the glenoid divided by the distance of the lateral humerus from the glenoid, A/H ( A ). The CSA is the angle from the lateral acromion to the inferior glenoid with respect to the glenoid fossa ( A ). The greater tuberosity angle is defined as the greater line from the superior humeral head to the superolateral edge of the humerus ( white arrows and line ) with respect to a line from center of the humeral head along the humeral diaphysis.
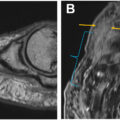
Two views of the left shoulder in a 68-year-old male. The AP view ( A ) demonstrates the LAA, depicted by the undersurface of the acromion ( black dotted line ) with respect to the glenoid fossa, and the ACEA, which is defined as the line from the center of the humeral head to the lateral acromial margins ( black arrows and line ) with respect to the glenoid fossa. The outlet view ( B ) shows a curved, or Type 2, acromion with identification of subacromial space (white marker).
Radiographic Measurements
Various radiographic measurements have been described. Although we do not report values, an understanding of thresholds and implications is important.
The acromiohumeral interval is the shortest linear distance between the acromial undersurface and the adjacent humeral head (see Fig. 1 A,C). This measurement should be performed on a neutral, true AP, or outlet view with 30° caudal views but has also been described on US and MR imaging. An acromiohumeral distance of ≤7 mm has been implicated in subacromial impingement and suggests supraspinatus tear.
The acromion index, measured on the AP view, is the distance of the lateral acromion to the glenoid divided by the distance of the lateral humeral head to the glenoid (see Fig. 1 A). The critical shoulder angle (CSA) defined as the line from the inferior glenoid to the lateral acromion with respect to glenoid fossa (see Fig. 1 A). The greater tuberosity angle, which is angle between a line from the superior humeral head to the superolateral edge of the humerus with respect to the humeral diaphysis has more recently been described (see Fig. 1 A). The acromiohumeral center edge angle (ACEA), which describes humeral head coverage by the acromion with respect to the glenoid has also recently been described (see Fig. 2 A). , A larger value for all of these measurements (0.7, 35°, 70°, and 18°, respectively) may be a risk factor for supraspinatus degeneration, though a low (<70°) lateral acromial angle (LAA) (undersurface of the acromion with respect to the glenoid fossa) may also be a factor (see Fig. 2 A). ,
Ultrasound
US is a well-tolerated and accessible imaging modality for evaluating shoulder impingement. Although US may have higher spatial resolution than MR imaging for superficial structures, the contrast resolution is inferior and intra-articular evaluation is limited. However, sonography allows for dynamic assessments that can directly correlate imaging findings with patient’s symptoms. While US of the shoulder has demonstrated excellent reliability, this is a highly operator-dependent modality with reliability and accuracy dependent upon user experience.
Diagnostic US of the shoulder should be performed with a high-frequency (9–17 MHz) linear transducer. Routine evaluation of the shoulder should include imaging of the structures outlined in Table 1 . Color or power Doppler imaging should be obtained routinely to exclude hyperemia at the proximal long head biceps tendon sheath, subacromial subdeltoid bursa, and glenohumeral and acromioclavicular joints. Additionally, any areas of perceived or suspected pathology should be interrogated with Doppler imaging. Although not requested at our institution, the coracoacromial ligament may also be identified sonographically.
Table 1
Routine protocol for ultrasound of shoulder impingement
| Anatomic Region | Dynamic Maneuvers | Doppler | Long-Axis and Short-Axis |
|---|---|---|---|
| Long head biceps tendon | + | + | |
| Subscapularis tendon | + | + | |
| Supraspinatus tendon | + | ||
| Infraspinatus tendon | + | ||
| Acromioclavicular joint | + | ||
| Subacromial-subdeltoid bursa | ∗ | + | |
| Posterior glenohumeral joint | + | ||
| Teres minor & infraspinatus muscle | |||
| Supraspinatus muscle |
∗Evaluation of the coracoacromial ligament may also be considered but is not requested at our institution.
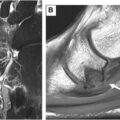
Each tendon should be imaged in long-axis and short-axis with greyscale imaging. Normal tendons are echogenic with fibrillar echotexture. Tendinosis is characterized by thickening, decreased echogenicity, and loss of normal echotexture ( Fig. 3 ). However, the curved morphology at the humeral head makes the rotator cuff tendons especially prone to anisotropy. Additionally, the interdigitating fibers at the infraspinatus-supraspinatus junction may artifactually appear pathologic. Attenuation of a tendon may reflect fraying or a more focal defined tear.
Diagnostic US of the left shoulder in a 65-year-old female. Severe supraspinatus tendinosis is demonstrated by an enlarged hypoechoic tendon with loss of normal architecture ( black arrow ). A superimposed near full-thickness tear with articular-sided and bursal-sided components is evidenced by anechoic fluid at the footprint ( white arrows ). Minimal residual tissue remains in continuity with productive bone ( black arrowhead ), and the tendon is not retracted.
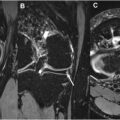
Real-time dynamic evaluation is the major strength of sonographic assessment. The choice of dynamic maneuver may be tailored to reproduce the patient’s pain, but forward flexion with abduction and internal rotation (similar to the Neer impingement test) is likely to be most sensitive. Hypoechoic thickening of the subacromial-subdeltoid bursa, fluid distention, and hyperemia are nonspecific findings ( Fig. 4 A ). However, pooling of bursal fluid or snapping of bursal tissue are positive findings for impingement. Bunching of the supraspinatus tendon or abutment of the greater tuberosity against the acromion may also be observed ,, (see Fig. 4 B).
Diagnostic US of the shoulder in a 58-year-old male with the transducer positioned anterior to the coracoacromial ligament. In the neutral position ( A ) no subacromial-subdeltoid thickening is appreciated. However, on abduction ( B ), there is bunching of the hypoechoic subacromial-subdeltoid bursa ( arrow ).
MR Imaging
MR imaging remains the gold standard for shoulder soft tissue evaluation due to its superior soft tissue contrast resolution, ability to evaluate osseous and intra-articular abnormalities, and absence of ionizing radiation. , Recent advances in MR imaging technology have improved spatial resolution and decreased acquisition times. However, relatively long examination times and patient discomfort and/or claustrophobia may contribute to motion degradation of image quality. Although radial sampling with oversampling the center of k-space may mitigate motion artifact, this technique provides suboptimal contrast and decreased image sharpness for intermediate-weighted imaging. When possible, imaging at 3-tesla (3T) is preferred over 1.5-tesla (1.5 T) as the increased signal typically affords improved image quality with faster acquisition times that help mitigate motion artifact.
Our routine protocol for the shoulder includes a single oblique coronal short inversion time inversion recovery (STIR) or T2-Dixon fat-suppressed sequence as well as straight axial, oblique coronal, and oblique sagittal intermediate-weighted 2-dimensional (2D) fast spin echo sequences ( Table 2 ). The patient is positioned supine with the arm to their side and thumb pointing up in a neutral position. If this position is too uncomfortable, then the patient may rest their palm on their abdomen with internal rotation at the glenohumeral joint. Most patients find a position in external rotation to be uncomfortable, so patients who relax into this position may have multidirectional instability ( Fig. 5 ). We do not perform MR arthrography because high-resolution noncontrast MR imaging has been shown to accurately define shoulder anatomy. T1-weighted imaging and the use of intravenous gadolinium-based contrast agents are generally reserved for the specific clinical questions regarding tumor or infection. Unexpected lesions may be interrogated with in-phase and opposed-phase T1-weighted Dixon imaging as intravoxel fat suggests benignity. Multiplanar gradient-recalled echo imaging can be obtained if there is concern for mineralization or hemosiderin deposition (eg, pigmented villonodular synovitis). Recent advances in 3-dimensional (3D) MR imaging have been well described noting reasonable scan times, increased through-plane resolution compared to 2D acquisitions, and the capacity for multiplanar reformation. ,, For skeletally immature patients, a 3D T1-weighted fat-suppressed physeal-sensitive gradient recalled sequence (SPGR) may also be obtained. Zero echo time (ZTE) is another 3D acquisition that can also provide CT-like contrast (see Fig. 5 ). However, for intermediate-weighted proton density (PD) imaging, we find the decreased in-plane resolution and suboptimal contrast resolution to be substantial limitations.
Table 2
Routine protocol for MR imaging of the shoulder
| Coronal Short Inversion Time Inversion Recovery | Axial Proton Density | Coronal Proton Density | Sagittal Proton Density | |
|---|---|---|---|---|
| TR (ms) | 4000 | 4000 | 4000 | 4000 |
| TE (ms) | 18 | 30 | 30 | 30 |
| FOV (cm) | 16 | 16 | 16 | 16 |
| Freq | 320 | 512 | 512 | 512 |
| Phase | 192 | 384 | 384 | 384 |
| Slice (mm) | 3 | 3 | 3 | 3 |
| Interslice gap (mm) | 0 | 0 | 0 | 0 |
| ETL | 14 | 14 | 14 | 14 |
| NEX | 1 | 1 | 1 | 1 |
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 High-Resolution Imaging of Knee Meniscus Anatomy and Tears
High-Resolution Imaging of Knee Meniscus Anatomy and Tears
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


