The peroneal tendons, composed of the peroneus longus and peroneus brevis tendons, play a critical role in foot biomechanics and ankle stability. Peroneal tendon abnormalities are commonly associated with chronic ankle instability and are major causes of lateral ankle pain. Early recognition and diagnosis of peroneal injuries can facilitate prompt treatment and management, leading to better patient outcomes and the prevention of long-term disabilities. Traditional ankle evaluation relies on 2D MR imaging sequences, which have limitations in the form of interslice gaps, partial volume effects, and orientation-dependent artifacts.
Key points
-
•
Peroneal compartment pathologic conditions are an important cause of lateral ankle pain that can be associated with chronic ankle instability.
-
•
Early recognition and diagnosis of peroneal compartment pathologic conditions with MR imaging can aid in prompt treatment and management, thus leading to better patient outcomes.
-
•
3D MR imaging of the ankle offers higher spatial resolution and improved fluid contrast that allows for better visualization of peroneal tendon pathologic conditions with the potential for better diagnostic performance compared with traditional two-dimensional sequences.
-
•
As high-resolution imaging of peroneal compartment pathologic condition plays an important role in surgical planning, structured image reporting with appropriate assessment criteria is critical for accurate diagnosis and management.
Abbreviations
| CPR | curved planar reconstruction |
| 2D | two-dimensional |
| 3D | three-dimensional |
| FSE | fast spin echo |
| IPR | inferior peroneal retinaculum |
| MPR | multiplanar planar reconstruction |
| PB | peroneus/peroneal brevis |
| PL | peroneus/peroneal longus |
| POPS | painful os peroneum syndrome |
| PQ | peroneus quartus |
| SPR | superior peroneal retinaculum |
| TSE | turbo spin echo |
Introduction
The peroneal tendons, comprising the peroneus longus (PL) and peroneus brevis (PB), travel from the lateral leg around the lateral malleolus, acting to evert and plantarflex the foot while stabilizing the lateral ankle. Peroneal tendon abnormalities can present as tenosynovitis, tendinopathy, tears, subluxation, and dislocation, commonly associated with chronic ankle instability, and represent one of the major causes of lateral ankle pain. Early recognition and diagnosis of peroneal injuries aid in prompt management, which can lead to better outcomes and prevention of long-term disability in patients.
The current standard of diagnostic imaging of chronic ankle instability based on the American College of Radiology’s Appropriateness Criteria is the radiograph as the first screening modality. If tendinopathy is suspected, MR imaging of the ankle without contrast or ultrasound of the ankle is the second-order modality. Although ultrasound offers a valuable and cost-effective tool for visualizing soft tissue abnormalities in the ankle region, MR imaging provides an excellent global anatomic detail and is a highly accurate tool for evaluating ligament and tendon pathologic conditions, as well as other possible internal joint derangement findings and myotendinous injuries. ,,
Traditional evaluation of the ankle relies on two-dimensional (2D) fast spin echo (FSE)/turbo spin echo (TSE) MR imaging sequences with images obtained in multiple predefined planes, and at times, lacking thin slices. 3D MR imaging sequences are being increasingly used in routine practices owing to higher resolution and multiplanar capabilities. There is a paucity of current literature showing detailed descriptions of peroneal tendon findings on three-dimensional (3D) MR imaging ( Tables 1 and 2 ).
Table 1
Institutional protocol for three-dimensional (intermediate-weighted) proton-density fat-suppressed MR imaging of the ankle
| Acquisition Plane | Slice Thickness/Gap (mm) | Pixel Size (F × P) (mm) | FOV (F × P) (mm) | TR (ms) | TE (ms) | Turbo Factor | Time of Acquisition (with Simultaneous Multislice Technique) |
|---|---|---|---|---|---|---|---|
| Sagittal |
1.5 T: 0.8 ISO/0
3.0 T: 0.7 ISO/0 |
Acquired ISO | 110 × 110 | 1100 | 40 |
1.5 T: 68
3.0 T: 55 |
1.5 T: 4.22 min
3.0 T: 5.43 min |
Table 2
Advantages of three-dimensional MR imaging of the ankle and foot versus two-dimensional MR imaging
| Structure of Interest | Relative Advantages of 3D Isotropic MR Imaging over 2D MR Imaging |
|---|---|
| Image quality | Higher signal-to-noise ratio, comparable contrast-to-noise ratio, improved image quality with less partial volume artifacts, less or no artifacts, improved fluid-contrast conspicuity, and reduced acquisition time compared with multiplanar 2D MR imaging |
| Ligaments | Better identification of variants, for example, split ligaments, intrasubstance ganglions, and distinguishing discontinuous ligament fibers from the adjacent scar tissue |
| Tendons | Specific tendon-aligned reconstructions. Improved identification of intrasubstance tears, split tears, and overall-tendon gaps with reduced magic angle artifacts |
| Hyaline cartilage | Better definition of cartilage layers, surface fissuring, and grade IV vs partial-thickness defects |
| Plantar plate | Specific plate-aligned reconstructions, especially in deformed or subluxed toes. Improved identification of partial, full-thickness, and partial-width tears |
| MR neurography | Vascular signal suppression with nerve-specific reconstructions and better identification of variations, for example, early branching and lesions along their axes |
The purpose of this article is to discuss the advantages of 3D MR imaging over 2D MR imaging in assessing detailed findings of peroneal tendon anatomic variations and pathologic conditions, along with illustrative examples. This article aims to improve the reader’s understanding of peroneal compartment lesions and assist radiologists in timely recognition and diagnosis of peroneal tendon abnormalities.
Normal anatomy
The two peroneal tendons, PL tendon and the PB tendon, are part of a larger peroneal complex consisting additionally of the peroneal tendon sheaths, the superior and inferior peroneal retinaculae (SPR and IPR), and frequently present accessory ossicle named, os peroneum , a sesamoid bone along the PL course. , The superficial peroneal nerve innervates the peroneal complex, and the peroneal artery provides blood supply with variable contributions of communicating branches of posterior tibial artery and anterior lateral malleolar branch of anterior tibial artery.
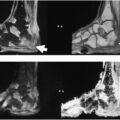
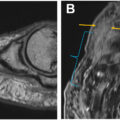
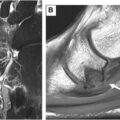
The PL originates from the head and upper two-thirds of the lateral fibula, the lateral condyle of the tibia, and the intermuscular septa and then runs distally within the lateral compartment of the leg. At the ankle, it routes posteriorly and inferiorly around the lateral malleolus through a common peroneal sheath, within the retromalleolar groove, a fibro-osseus tunnel formed by the SPR, the posterior inferior tibiofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament ( Fig. 1 ). Distally, the PL passes below the peroneal tubercle of the lateral calcaneus, within its own synovial sheath. The tendon then travels on the plantar aspect of foot, anteromedially through the cuboid groove, and inserts into the plantar side of the first cuneiform and the base of the proximal first metatarsal.
( A ) The PL and PB tendons, SPR, and IPR. ( B ) Illustration adapted from Kumai and Benjamin showing the anatomic and histologic structure of the malleolar groove. The SPR attaches to a periosteal fibrocartilage (periosteal fc) at the posterior aspect of the fibula forming an osteofibrous tunnel containing the PL, PB, distal peroneal brevis muscle (PB muscle), and common peroneal tendon sheath (CPT sheath). Note the intricate relationship of the groove and posterior talofibular ligament (PTF lig). ( C ) FSE 3D T2 fat-saturated MR imaging (first column on panel C), 2D DIXON PD water only (second column), and in phase (third column) demonstrating PB ( long arrow ) and PL ( short arrow ) on slices corresponding to levels shown on panel B. PB; PL; SPR.
More inferiorly, the PB originates from the lower two-thirds of the lateral fibula and the intermuscular septum. It courses anteromedially alongside the PL in a common sheath around the lateral malleolus. It has a muscle belly as compared with PL at ankle level. Distally, the PB crosses above the peroneal tubercle within its own synovial sheath ahead of PL (brave), remains lateral, and inserts into a tuberosity on the lateral side of the fifth metatarsal as apposed to the lateral cord of the plantar fascia, which inserts at the tip of the base of the fifth metatarsal (see Fig. 1 ).
Branches from the peroneal and anterior tibial arteries supply 1 to 2 vincula that vascularize each peroneus tendon from the posterolateral side. , There is controversy in the literature whether the medial or lateral tarsal arteries contribute to the peroneal tendons vasculature. Although the literature agrees that the peroneal tendons are overall well vascularized, there is disagreement about the presence of avascular zones in the posterior malleolus, the retromalleolar groove, the cuboid groove, and the tendon insertion, as these zones are frequent locations of tendon tears. Furthermore, there is also disagreement about which tendon has more avascular zones or if they even have them at all. The PL and PB tendons pass from the leg to the foot by wrapping around the lateral malleolus. As they turn around this bony pulley, they lie in a fibro-osseous tunnel. The concept of wrap-around tendon applies to both PTs; therefore, variable amounts of fibrocartilage can be present in zones of compressive forces, such as the retromalleolar and cuboid grooves (see Fig. 1 ).
Anatomic variations in the peroneal compartment include an enlarged peroneal tubercle, which normally functions to divide the PL and PB tendons. The increased size of the tubercle leads to friction and inflammation of the peroneal tendon sheath, associated with tenosynovitis and partial tears. The retrotrochlear eminence is another anatomic protuberance on the lateral calcaneus that is located posterior to the peroneal tubercle and tendons. Hypertrophy of eminence is also frequently associated with an accessory muscle, peroneus quartus (PQ). ,,
Accessory peroneus muscles are common anatomic variations, with the PQ being the most common, as it has been estimated to exist in 12% to 22% of the population. , The PQ originates at the distal lateral portion of the fibula and can insert at various sites, commonly the retrotrochlear eminence or the PL tendon. Although the presence of the PQ is largely asymptomatic, it can cause crowding at the retrotrochlear groove and thus potentially predisposes to subluxation/dislocation and tears of the PB tendon. , PQ or anteriorly located peroneus tertius can also be used as tendon graft or for tendon transfer surgery.
A low-lying PB muscle belly is another variation described as an extension of the muscle tissue distal to the tip of the fibula. This can be asymptomatic or can cause crowding of the retromalleolar groove and peroneal sheath, increasing tendon strain and laxity of the SPR, predisposing to peroneal tears/subluxation. , Another variation could be the bifid PB tendon, which could be mistaken for a pathologic split.
The presence of an os peroneum , a sesamoid bone within the PL tendon located near the cuboid, has been associated with PL pathologic condition, presumably secondary to tendon degradation and increased risk of injury. Abnormalities of the ossicle itself are also seen, with edema, fracture, or diastasis of bipartite os peroneum, known as “ os peroneum syndrome.”
Variations in the retromalleolar groove shapes are also common among the general population. These can present morphologically as a concave (usually <1–1.5 mm) groove above the lateral ankle joint, a flat or convex groove, or an irregular groove. The latter two groove shapes and deficient SPR can predispose patients to peroneal tendon subluxations/dislocations and tears. The peroneal groove can also develop lateral traction spurs from the groove. It should be noted that intrasheath subluxations of PL/PB tendons are easily evident on dynamic ultrasound owing to real-time capabilities and can be missed on MR imaging. However, kinematic MR imaging is useful for finding subluxation or dislocation of the PL with higher soft tissue contrast.
Physiology and biomechanics
The ankle and hindfoot joints are formed by the talocrural, subtalar, and talocalcaneonavicular articulations, the arc of motion of which includes plantar flexion and dorsiflexion, inversion and eversion, and abduction and adduction. Combinations of these movements lead to the 3D motions of supination and pronation, in which the sole of the foot faces medially or laterally, respectively. As discussed above, the PTs originate on the lateral side of the leg and run posterior-inferiorly around the lateral malleolus. They function to evert and plantarflex the foot and provide lateral ankle stability. ,
The role of the PTs depends on the shape of the foot, which is categorized mainly by the shape of the medial longitudinal arch and the hindfoot. The arch can be high (pes cavus), neutral (rectus), or low (pes planus). Although the posterior tibialis tendon plays a greater role in maintaining the medial arch, Kokubo and colleagues , found that the PL reduces sagittal first metatarsocuneiform joint subluxation, improves the intermetatarsal angle during weight bearing, and stabilizes the proximal transverse arch of the foot. As such, PL tears and dysfunction affect the integrity of the arch and have been associated with pes cavus–adductus deformity. ,
The PL assists the windlass mechanism by enhancing dorsiflexion of the first metatarsophalangeal joint during the midstance phase of walking by plantarflexing the forefoot, everting the hindfoot, and keeping the first ray gripped to the ground. The windlass mechanism happens when the plantar fascia and the flexor hallucis longus are in equilibrium. This generates potential energy owing to elasticity. This potential energy is converted to kinetic energy during propulsion when the first metatarsophalangeal joint dorsiflexes, and the foot raises off the ground to take a step.
Pathologic condition and two-dimensional–three-dimensional MR imaging findings
Normal MR Imaging, MR Imaging Protocols, and Imaging Pitfalls
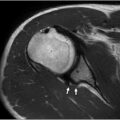
Normal peroneal tendons display low-signal intensity on MR imaging. The PB fits within the fibular retromalleolar groove and thus typically appears flat or mildly crescentic, which should not be interpreted as a split tear (see Fig. 1 ). The PL presents as a more globular or oval cross-sectional shape (see Fig. 1 ). , Increased signal intensity of the peroneal tendon is usually associated with tendon pathologic condition, especially if the tendon is enlarged, but can also be secondary to technical pitfalls, such as the magic angle effect, which is reduced on higher echo time values. , Mild plantarflexion of the foot at a 20° angle when imaging helps mitigate this problem. ,,,,
Artifacts resulting from the magic angle effect are particularly pronounced on 2D MR imaging acquisition, which might require an additional T2 axial or coronal oblique sequence to be added to the standard protocol to increase accuracy and reliability, at the expense of longer examination times. As such, 2D MR imaging possesses several limitations, including larger slice thickness, pulsation artifacts especially if high echo spacing, partial volume effects associated with interslice gaps, and, as mentioned, longer examination times to acquire additional planes. Consequently, high-resolution 3D MR imaging sequences, such as 3D TSE with longer echo trains, are gaining popularity because of their advantages over 2D MR imaging. The 3D MR imaging sequence is acquired as a volume scan with thin slice reconstructions and without interslice gaps, thus allowing multiplanar isotropic high-resolution reformats. In addition, 3D sequencing allows tendon-specific reconstructions with creation of a true-tendon axial plane that better visualizes small tears around the lateral malleolus tip, thereby offering a more complete picture of the peroneal tendon lesions. This also mitigates the need for additional image acquisition, thus reducing the overall duration the patient must spend in the scanner. The excellent anatomic detail and improved fluid contrast that are characteristic of 3D MR imaging allow for better visualization of tendon pathologic conditions, such as split tears and tendon gaps, in the context of complete tears. However, as 3D TSE sequences reduce effective echo time (TE), these benefits may come at the expense of more prominent magic angle artifacts. ,, Nevertheless, a study by Duarte Silva and colleagues suggests that the combination of a higher acceleration with 3D TSE sequences can address many of the shortcomings of 3D MR imaging while also offering equal or better diagnostic performance when compared with 2D TSE.
Conversely, it is imperative to acknowledge potential limitations associated with the utilization of 3D MR imaging sequences. These limitations primarily manifest in the time required for reconstruction based on the expertise of the radiologist and the capabilities of the workstations and software used. Given early stages of 3D MR imaging usage in joint assessment, it has been integrated as an additional sequence to conventional 2D protocols; this integration may result in extension of the protocol’s duration. Moreover, reducing time for these 3D sequences or even patient’s movement can lead to undesired acquisition artifacts. With the use of fast parallel imaging, the 3D acquisition of the ankle only requires 3 minutes of gradient time on 3-T scanners and 4 minutes on 1.5-T scanners. Typical parameters include repetition time (TR) = 1000 to 1100 ms, TE = 35 to 45 ms, fat suppression = spectral attenuated inversion recovery, and isotropic voxel = 0.7 mm with sagittal plane volume acquisition on both 1.5-T and 3-T scanners. The voxel size can be increased to 0.8 mm isotropic in large patients. Further enhancements using artificial intelligence on the horizon are expected to reduce the imaging times with preservation of the image quality (see Table 1 ).
Peroneal Tendinopathy and Tenosynovitis
Peroneal tenosynovitis refers to inflammation and fluid within the tendon synovium, and tendinopathy is the degeneration of the tendon collagen fibers. These conditions are caused by overuse of the PTs from repetitive or prolonged activity and are commonly seen in ballet dancers; runners; patients who increase their physical activity suddenly after a long period of rest, secondary to fractures and sprains; and patients with chronic lateral ankle instability. ,,, Chronic lateral ankle instability is a common pathologic condition affecting at least 20% of patients that experienced lateral ankle sprain and is defined as pain lasting more than 6 weeks after an acute episode. ,
The association between lateral ankle instability and peroneal injuries underscores the significance of a comprehensive evaluation of the lateral ankle ligaments in these patients. Typically, it primarily affects the anterior talofibular ligament and the calcaneofibular ligament. Repeated ankle sprains lead to laxity and attenuation of the SPR and the peroneus tendons as blood supply to the retinacular groove is compromised, increasing the risk of tendinopathy and tears.
On MR imaging, peroneal tendinopathy appears as intermediate diffuse increased signal with potential tendon thickening or fraying. As a rule, the tendons from largest to smallest diameters at the ankle are tibialis posterior, tibialis anterior, and PL, respectively. If PL is larger than either of the other two mentioned tendons, it can be classified as PL tendinopathy, especially if there is some increased signal. Any fluid-bright signal or focal split/discontinuity would be a focal tear. Although some fluid within the tendon sheath is considered normal, greater than 3 mm of circumferential fluid distending the common peroneal tendon sheath is indicative of tenosynovitis on MR imaging. Greater than 2 mm of fluid surrounding the PB or PL would similarly suggest tenosynovitis of the corresponding tendon, especially with sheath thickening, internal septations, or debris. , Contrast MR images may reveal active inflammation and contrast enhancement of the synovium. Notably, the presence of fluid accumulation in the common peroneal tendon sheath from a calcaneofibular ligament tear can be mistaken for tenosynovitis. Therefore, it is important to examine and rule out tears of the lateral collateral ligaments before considering tenosynovitis. ,
Stenosing tenosynovitis, which is caused by subacute-chronic synovial proliferation and fibrosis surrounding and restricting the peroneal tendons, presents on MR imaging as thickened synovium with intermediate- or low-signal-intensity multiple linear septations and/or loculations within the synovial fluid. These findings can be seen on all MR imaging pulse sequences. ,
Moreover, patients with enlarged bone protuberances, low-lying brevis muscles, and accessory PQ tendons are at increased risk, as these conditions lead to stenosis of the tendon sheath and increased friction. On MR imaging, an enlarged peroneal tubercle is considered when higher than 5 mm relative to the lateral calcaneal cortex. , Taneja and colleagues showed that using a cutoff of 4.3 mm for an enlarged peroneal tubercle presents higher correlation with peroneal tenosynovitis and partial tears, with sensitivity and specificity reaching greater than 70%. The PB muscle belly can vary in how much the musculotendinous junction extends past the fibular tip. Therefore, a low-lying PB muscle belly is only diagnosed when the myotendinous junction extends 15 mm or greater distal to the tip of the fibula on MR imaging. Notably, this anatomic variation can present differently depending on foot position, with greater extension during dorsiflexion and less commonly with plantarflexion. ,,,
On MR imaging, accessory PQ muscles are best visualized in the axial plane. The PQ is isointense relative to other muscles and is located posteromedial to the peroneal tendons as a distinct structure that is separated from adjacent peroneal muscles by a fat plane. ,, Length and thickness of the PQ tendon is highly variable, with some tendons with very thin morphology. Thicker tendons can be more easily visualized on both fat-saturated and non–fat-saturated sequences, whereas thin tendons are better depicted on non–fat-saturated sequences. A detailed description of such characteristics can be added by the surgeon in cases with potential need for tendon graft and tendon transfer. As the PQ can have variable insertions, it can be mistaken for a PB tendon tear in situations of close approximation or fusion of the PQ tendinous slips with the PB tendon. The PQ muscle can also be mistaken for a low-lying PB muscle belly. Therefore, it is imperative to corroborate the findings of an accessory PQ muscle with high-resolution imaging visualization of the PQ muscle axially to its insertion site. ,,,
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 Wrist Ligaments Injuries and Instability
Wrist Ligaments Injuries and Instability
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


