Wrist instability is a challenging topic for radiologists due to the wrist’s intricate ligamentous anatomy and complex kinematics. This article provides a comprehensive overview of the intrinsic and extrinsic wrist ligaments, their characteristic imaging appearance, and the pathomechanics and classification systems of carpal instability to enhance radiologists’ ability with the diagnosis of wrist ligamentous pathologies. Furthermore, the evolving role of advanced imaging modalities, such as high-resolution MR, kinematic MRI, MR arthrography, 4DCT, CT arthrography, and dynamic imaging techniques for the assessment of the wrist biomechanics and detecting subtle ligamentous injuries were detailed.
Key points
-
•
Assessment of the intrinsic and extrinsic wrist ligaments is critical for diagnosing carpal instability patterns.
-
•
High-resolution MR, MR arthrography, CT arthrography, cineradiography, and dynamic fluoroscopy are essential tools in evaluating wrist ligament pathology.
-
•
Novel technologies, such as 4DCT and dynamic MR imaging are enhancing the evaluation of wrist kinematics, offering promising avenues for early and precise detection of instability.
Abbreviations
| 2D | 2-dimensional |
| 3D | 3-dimensional |
| 4D | 4-dimensional |
| CBCT | cone-beam computed tomography |
| CI | confidence interval |
| CIC | carpal instability complex |
| CID | carpal instability dissociative |
| CIND | carpal instability nondissociative |
| CT | computed tomography |
| CTA | computed tomography arthrography |
| DIC | dorsal intercarpal |
| DISI | dorsal intercalated segmental instability |
| DRUJ | distal radioulnar joint |
| DRUL | distal radioulnar ligament |
| ECU | extensor carpi ulnaris |
| FDA | Food and Drug Administration |
| FSE | fast spin echo |
| MPR | multiplanar reconstruction |
| MRA | MR arthrography |
| PA | posteroanterior |
| PD | proton density |
| RF | radiofrequency |
| SC | scaphocapitate |
| SLAC | scapholunate advanced collapse |
| SNR | signal-to-noise ratio |
| STT | scaphotrapeziotrapezoid |
| TFC | triangular fibrocartilage |
| TFCC | triangular fibrocartilage complex |
| THC | triquetro-hamate-capitate |
| VISI | volar intercalated segmental instability |
Video content accompanies this article at http://www.radiologic.theclinics.com .
Introduction
Wrist instability is a challenging topic for many radiologists due to the complexity of anatomy, kinematics, and the various patterns of instability that can occur. The wrist is composed of 20 articulations and stabilized by many ligaments with multiple connections to the radius, ulna, carpal bones, and metacarpal bases. Imaging is essential to the diagnosis and management of wrist instability; thus, radiologists have the unenviable task of assessing these complex structures to accurately diagnose the injury pattern and guide treatment. Wrist instability is associated with pain, loss of motion, and, if left untreated, can lead to osteoarthritis and a significant loss of function. Recent advances in imaging have enhanced the visualization and assessment of wrist ligament injuries. This article will focus on advanced imaging of the ligaments central to wrist stability.
Intrinsic ligaments of the wrist
The wrist ligaments are broadly categorized into intrinsic and extrinsic ligaments. Intrinsic wrist ligaments are those that originate and insert on the carpal bones. Conversely, the extrinsic wrist ligaments connect the forearm to the carpal bones and may have additional attachments to retinacula and/or the tendon sheaths. , The most clinically important intrinsic ligaments are the scapholunate and lunotriquetral ligaments. ,
Scapholunate ligament
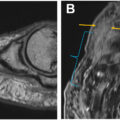
The scapholunate ligament is a horseshoe or “u-shaped” ligament and is the primary stabilizer of the scapholunate joint. It is composed of 3 components—the dorsal, volar, and proximal bands ( Fig. 1 ). The dorsal and volar bands are both categorized as “true ligaments” as they are primarily composed of collagen fibers. The dorsal band is the most biomechanically important component for scapholunate stability, measuring approximately 3 mm in thickness, and contributes to the tensile strength of the scapholunate joint. In comparison, the volar band is longer and thinner, measuring approximately 1 mm in thickness, and is therefore weaker than the dorsal band. The proximal component is composed of fibrocartilaginous membrane and does not significantly contribute to wrist stabilization.
U-shaped scapholunate ligament with the volar ( blue ), proximal ( yellow ), and dorsal ( purple ) components.
Lunotriquetral ligament
The lunotriquetral ligament, much like the scapholunate ligament, is a horseshoe-shaped ligament composed of 3 components—the dorsal, volar, and proximal bands. Its function is to provide stability to the proximal carpal row and serves as the primary stabilizer of the lunotriquetral joint. In contrast to the scapholunate ligament, the volar component of the lunotriquetral ligament is the thicker and stronger band, measuring 2 mm in thickness and resists volar and dorsal translation. The dorsal band is thinner, measuring 1 mm; its function is to resist flexion, extension, and rotation. , When compared with the scapholunate ligament, the lunotriquetral ligament is less flexible, resulting in less potential for movement at the lunotriquetral joint.
Midcarpal intrinsic ligaments
Additional intrinsic midcarpal ligaments, such as the triquetro-hamate-capitate (THC), scaphocapitate (SC), and scaphotrapeziotrapezoid (STT) ligaments, contribute to stability at the midcarpal joint as well as secondary stability to the proximal carpal row ( Fig. 2 ). On the dorsal side, there is a midcarpal ligament called the dorsal intercarpal (DIC) ligament, comprising the dorsal triquetroscaphoid and the triquetrotrapezoid-trapezial ligaments, which connect the triquetrum and the distal scaphoid and contribute to secondary stabilization of the wrist ( Fig. 3 ). Additionally, the dorsal capsular scapholunate septum, a fibrous structure that connects the dorsal band of the scapholunate ligament to the DIC, also contributes to secondary stabilization; however, it is variably seen on imaging.
Intrinsic midcarpal ligaments: Coronal oblique PD 3D cube ( A and B ) MR images demonstrating the intrinsic midcarpal ligaments of the wrist.
Dorsal ligaments: Coronal ( A ) and axial oblique PD ( B and C ) MR images of the wrist demonstrating the intrinsic DIC ligament and extrinsic dorsal radiotriquetral ligament (DRT).
Extrinsic ligaments of the wrist
The extrinsic ligaments are critical secondary wrist stabilizers. Injury to these ligaments may produce chronic wrist pain and contribute to wrist instability. Broadly, the extrinsic ligaments can be further categorized into the volar and dorsal extrinsic ligaments.
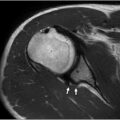
The most significant volar extrinsic ligaments are the radioscaphocapitate, long radiolunate, and short radiolunate ligaments ( Fig. 4 ). On the radial and volar aspect of the wrist, these ligaments form a “V” shaped structure. The volar ligaments are thicker and stronger when compared with the dorsal side.
Volar extrinsic ligaments: Coronal PD cube ( A ) and sagittal T1 fat saturated (FS) ( B ) MR images demonstrating volar extrinsic ligaments. LRL, long radiolunate ligament; RSC, radioscaphocapitate; SRL, short radiolunate ligament.
The most significant dorsal extrinsic ligament is the dorsal radiotriquetral, or radiocarpal ligament. Together with the intrinsic dorsal intercarpal ligament, the dorsal wrist ligaments are orientated in a “V” shape, rotated 90° (see Fig. 3 ). This structure is crucial for allowing the controlled movement of the scaphoid imaging. Fig. 5 and Table 1 summarize the anatomy, function, and pathology of the wrist ligaments.
Secondary stabilizers of the wrist: volar (left) and dorsal (right) ligaments.
Table 1
Carpal ligaments
| Ligament | Origin | Insertion | Function | Pathology |
|---|---|---|---|---|
| Volar extrinsic ligaments | ||||
| Radioscaphocapitate ligament |
Volar distal radial styloid
Scaphoid tuberosity |
Volar tubercle of the capitate |
Stabilizes the midcarpal joint
Prevent the scaphoid from dorsal subluxation Keeps the scaphoid in a volar flexed position |
Injury can contribute to radiocarpal CIND with ulnar translocation
Injury can contribute to midcarpal CIND-DISI |
| Long radiolunate ligament | Volar and medial margin of the distal radial styloid | Radial margin of the volar surface of the triquetrum | Stabilizes the lunate Prevent dorsal flexion and volar translocation | Injury, in combination with scapholunate or lunotriquetral ligament tears, can contribute to CID DISI or VISI, respectively |
| Short radiolunate ligament | Volar rim of the lunate fossa of the radius | Proximal radial part of the volar surface of the lunate | Stabilizes the lunate | Injury, in combination with lunotriquetral ligament tears, can contribute to CID VISI |
| Dorsal extrinsic ligaments | ||||
| Dorsal intercarpal ligament | Dorsal ridge of the triquetrum | Dorsal distal lunate and dorsal groove of the scaphoid |
Secondary stabilizer of the wrist
Unites the triquetrum and distal scaphoid |
Injury can contribute to midcarpal instability |
| Dorsal radiotriquetral ligament | Distal radius at Lister’s tubercle and/or the styloid process of the radius | Dorsal tubercle of the triquetrum Dorsal lunate |
Secondary stabilizer of the carpal bones
Limits intracarpal supination, radial deviation, volar flexion, and ulnar translation Stabilizes the lunate in volar flexion |
Injury can contribute to carpal instability |
| Intrinsic ligaments | ||||
| Scapholunate ligament | Dorsal, volar, and proximal scaphoid | Dorsal, volar, and proximal lunate | Primary stabilizer of the wrist | CID scapholunate dissociation, DISI, and SLAC |
| Lunotriquetral ligament | Dorsal, volar, and proximal lunate | Dorsal, volar, and proximal triquetrum | Primary stabilizer or the wrist | CID lunotriquetral dissociation, VISI |
| Triquetral-hamate-capitate (THC) ligament | Volar side of the triquetrum | Volar and ulnar side of the capitate |
Stabilizer of the midcarpal joint
The thickest midcarpal ligament |
Injury can contribute to midcarpal CIND-VISI |
| Scapho-trapezio-trapezoid (STT) ligament | Volar and dorsal aspect of the distal pole of the scaphoid | Trapezium and trapezoid | Stabilizer of the distal pole of the scaphoid, trapezium, and trapezoid | Injury, in combination with scapholunate ligament tear, can contribute to CID with progression to DISI and SLAC |
Abbreviations: CID, carpal instability dissociative; CIND, carpal instability nondissociative; DISI, dorsal intercalated segmented instability; SLAC, scapholunate advanced collapse; VISI, volar intercalated segmented instability.
Pathology
Carpal Instability
Carpal instability occurs when the wrist joint cannot maintain its normal alignment as it moves under physiologic loads. It can occur secondary to traumatic injury, inflammatory arthritis, infection, and/or congenital abnormalities.
The Mayo classification describes patterns of carpal instability as “dissociative” and “nondissociative.” Carpal instability dissociative (CID) is a static or dynamic malalignment between the carpus within the same carpal row. Carpal instability nondissociative (CIND) is structural or dynamic malalignment of the radiocarpal joint or midcarpal joint with preserved structural and dynamic alignment of the joint spaces within the same carpal row. The carpal instability complex (CIC) pattern features findings of both CID and CIND.
Carpal Instability Dissociative: Intracarpal Row Instability
CID can be further subdivided into predynamic, dynamic, or static. Predynamic instability may not be detected on standard plain radiographs, stressed views, or cineradiography. However, it can be diagnosed by arthroscopy and on kinematic 4 dimensional (4D) CT, or kinematic MR arthrography (MRA). Dynamic instability is visible on stress views and cineradiography but not seen on standard radiographic views. Static instability is present even on standard radiographs, indicating significant failure of primary and secondary wrist ligaments.
Proximal dissociative instability is the most common form of CID. Distal dissociative instability is much less common, with the distal carpal rows split into columns from a high-energy crush or blast injury. Distal dissociative instability is beyond the scope of this discussion.
Proximal Dissociative
The most common proximal CID pattern is scapholunate dissociation. Scapholunate dissociation is a spectrum of pathology related to abnormal alignment and movement at the scapholunate joint. It commonly occurs after trauma, classically after a fall onto an extended hand in ulnar deviation. The initial predynamic form of scapholunate instability occurs from tearing of the volar and proximal components of the scapholunate ligament. Subsequent tearing of the dorsal component will result in dynamic instability. If left untreated, involvement of the secondary stabilizers, including the midcarpal intrinsic, dorsal, and volar extrinsic ligaments, will lead to static instability and carpal malalignment known as dorsal intercalated segmental instability (DISI), ultimately progressing into scapholunate advanced collapse (SLAC).
By contrast, lunotriquetral dissociation is less common than its scapholunate counterpart. Lunotriquetral tears can also lead to dynamic and static instability. A disruption in Gilula first arch or subtle lunotriquetral widening can suggest ligamentous injury on radiographs. Tears of the lunotriquetral ligament and secondary stabilizers such as the dorsal radiotriquetral ligament and long radiolunate ligament then lead to increased palmar flexion of the lunate, or volar intercalated segmental instability (VISI).
Imaging of carpal instability
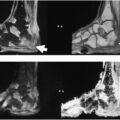
Radiographs still play a pivotal role in the initial evaluation of wrist pain, including ligament injuries, and are the initial diagnostic modality for evaluating wrist pain. Radiographs provide ancillary findings that help differentiate the etiologies of wrist pain, such as osseous fractures, static wrist instability, infection, arthritis, or tumors. Thus, it can be utilized as a triage tool for patients with wrist pain, specifically in those suspected of having a scapholunate ligament injury. The standard posteroanterior (PA) and lateral views can delineate the indirect signs of lunotriquetral and scapholunate interosseous ligament tears, including the carpal angle abnormalities (DISI/VISI) on the lateral view and increased space between carpal bones. On the PA radiograph, Gilula’s arcs should be parallel without discontinuity or step-off, the carpal bones should have apposing bone surfaces less than 2 mm, and a normal scapholunate distance should measure no more than 3 mm. On the standard lateral view, DISI appears as an increased scapholunate angle greater than 60°, an increased lunocapitate angle greater than 30°, and an increased radiolunate angle greater than 15°. In VISI, the lunocapitate angle is increased to greater than 30° while the scapholunate angle is less than 30° ( Fig. 6 ). It is often helpful to compare the alignment to the contralateral wrist.
PA radiograph ( A ) of the wrist outlining Gilula’s arcs, which should be parallel without discontinuity or step-off. Lateral radiograph ( B ) demonstrating scapholunate ( light orange ) and lunocapitate ( dark orange ) angles.
When the standard static radiograph is normal but carpal instability is suspected, a stress radiograph should be obtained. However, it should be utilized with caution as it may exacerbate ligament injury. These views can be obtained as a PA view with the wrist in clenched fist view, ulnar, or radial deviation views—with ulnar deviated views highlighting injuries to the scapholunate ligament and radial deviated views highlighting injuries to the lunotriquetral ligament. Diastasis greater than 3 mm is indicative of ligament disruption. Less commonly used stress radiographs include lateral views with the wrist in flexion and extension, which can help detect both dynamic and static scapholunate instability and midcarpal instability. Cineradiography, dynamic fluoroscopic imaging, or 4DCT allows for visualization of the osseous structures, alignment, and kinematics while undergoing dynamic maneuvers, including flexion-extension, radial-ulnar deviation, as well as the dart-thrower’s motion—the arc of motion from radial deviation and wrist extension to ulnar deviation and wrist flexion. Dynamic imaging is particularly useful for the evaluation of a “click,” “clunk,” or “snapping” phenomenon ( [CR] ).
Computed tomography (CT) arthrography (CTA) of the wrist, using the 3-compartment injection and obtaining thin-slice reformatted images, can provide a more accurate assessment of interosseous ligament injuries ( Fig. 7 ). The diagnostic performance of CTA in the diagnosis of wrist ligament tears has been reported differently in the literature. For example, the sensitivity and specificity of CTA in the diagnosis of scapholunate interosseous ligament tears ranged from 58% to 100% ,, and 79% to 100%, ,, respectively. A recent meta-analysis that evaluated the accuracy of cone-beam computed tomography (CBCT) arthrography in diagnosing wrist ligament injury reported a sensitivity and specificity of 93% (95% confidence interval [CI] 40–100) and 91% (95% CI 81–96), respectively, for scapholunate ligament injuries and a sensitivity and specificity of 83% (95% CI 37–98) and 64% (95% CI 42–81), respectively, for lunotriquetral ligament injuries. Some authors have found that CTA is superior to MRA in the diagnosis of intrinsic wrist ligament partial tears. , Chhabra, Shores, and Demehri demonstrated the benefit in utilizing 4DCT to assess wrist instability after ligament repair, which can show mild persistent diastasis in stable repairs but no disruption of Gilula’s arc or step off on dynamic CT.
Scapholunate tear: CT arthrogram coronal image through scapholunate interval demonstrates widening with contrast extending into the interval compatible with communicating tear.
Nevertheless, MR imaging is still the most sensitive modality for evaluation of wrist ligaments. Because of the complexity and small size of wrist ligaments, it is essential to obtain high-resolution images (in-plane resolution 0.5 mm) with high signal-to-noise ratio (SNR) intermediate-weighted imaging; thus, the higher magnet strengths, such as 3 Tesla (3T) are preferred. The introduction of multichannel coils with a higher number of receivers and 3-dimensional (3D) sequences also contributes to improved imaging evaluation. Isotropic 3D imaging has several advantages compared with high-resolution 2-dimensional (2D) sequences, including permitting multiplanar reconstruction (MPR), acquisition of images with thin sections smaller than 1 mm (usually 0.6–0.7 mm), allowing accurate cross-referencing of small structures without misregistration, reduction of volume averaging associated with 2D imaging, and potential time savings with obtaining a single 3D sequence. Intra-articular contrast injection and performing MRA is another technique for increasing the diagnostic accuracy of wrist ligamentous pathologies. In a study on 22 patients by Cherian and colleagues, the sensitivity, specificity, and diagnostic accuracy of MR imaging in the diagnosis of the scapholunate interosseous ligament were 75%, 100%, and 95.4%, respectively, while the sensitivity, specificity, and diagnostic accuracy of MRA were 100%, 100%, and 100%, respectively. In a meta-analysis by Hafezi-Nejad and colleagues that compared the diagnostic performance of MR imaging and MRA for the diagnosis of scapholunate interosseous ligament by inclusion of 24 studies, MRA had higher sensitivity (82.1% [95% CI 76.1–87.2] vs 75.7% [95% CI 66.8–83.2]) but less specificity (92.8% [95% CI 90.2–94.9] vs 97.1% [95% CI 89.8–99.6]) than 3T MR imaging.
MR imaging appearance
Fluid-sensitive fat-suppressed sequences are the best sequences in the depiction of ligament injuries. Due to the U-shaped structure of the scapholunate and lunotriquetral intrinsic ligaments, the dorsal and volar components are best seen on axial sequences, while the proximal components are best visualized on coronal sequences ( Figs. 8 and 9 ). The dorsal and volar components of the scapholunate and lunotriquetral ligaments should demonstrate homogenous low signal on spin-echo images. 3D gradient-echo sequences may reveal variable signal intensity, particularly in the volar component of the scapholunate ligament. The proximal components may have a triangular or wedge shape on coronal images and can show variable signal intensity. It should be noted that solitary central perforations of the ligament components are typically degenerative in etiology and generally not painful.
Normal scapholunate ligament on MR: coronal ( A ) and axial ( B ) T1 FS MRA images showing intact dorsal ( green arrow ), volar ( red arrow ), and proximal ( yellow arrow ) components of the scapholunate ligament.
Normal lunotriquetral ligament on MR: coronal ( A ) PD FS SPACE (3D) and axial ( B ) MPR images demonstrating the dorsal ( green arrow ), volar ( red arrow ), and proximal ( yellow arrow ) components of the lunotriquetral ligament.
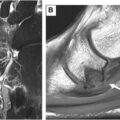
Visualization of scapholunate dissociation (scapholunate distance > 3 mm), soft tissue ganglion formation, and avulsive cystic changes at the osseous attachment of the scapholunate interosseous ligament components are suggestive of a ligament tear. Ligament tears may be described as complete or incomplete depending on the involvement of all or only some components of the ligament and as full-thickness or partial-thickness tears of individual ligamentous bands. Partial tears of the interosseous ligaments are appreciated as altered signal intensity, contour irregularity, or focal thinning, while complete interosseous ligament tears demonstrate morphologic distortion or distinct areas of ligament discontinuity. A ligament stump can be appreciated at the scaphoid or lunate site of detachment as hanging free. In MRA, a ligamentous tear could be appreciated as contrast extravasation into the midcarpal compartment, periligamentous infiltration, nonvisualization and discontinuity of ligament, contour irregularity with waviness, or changes in signal intensity ( Figs. 10 and 11 ). Secondary signs of ligament injury include scapholunate or lunotriquetral disassociation, arch disruption, and soft tissue ganglion or intra-osseous ganglion cyst formation. In the chronic phase of tears, fibrous thickening or scarring can limit identification of tears on arthrography due to a lack of contrast imbibition or extravasation.
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


