CASE 34 Anthony G. Ryan and Peter L. Munk A 22-year-old woman presented with chronic, worsening pain in her midfoot, exacerbated by, and now limiting participation in, recreational dance classes. Figure 34A Figure 34B Figure 34C Figure 34D A lateral foot radiograph (Fig. 34A) demonstrates loss of definition of the posterior navicular wall and an elongated anterior process of the calcaneum, with an apparent bony bar extending between the two bones. Sagittal MPGR images (Figs. 34B, 34C) demonstrate a clear union between the anterior calcaneum and posterior navicular. The junction between the two bones is of higher signal intensity than the adjacent cortex. The margins of the junction demonstrate irregular low signal intensity encroaching on the higher signal region. The higher signal intensity does not reach that of cartilage. A coronal T2-weighted fat-saturated image (Fig. 34D) shows contiguity of the calcaneum and navicular at this site (arrow). Calcaneonavicular coalition (partially ossified fibrous union). Acquired intratarsal ankylosis secondary to infection, trauma, arthritis, or surgery. Tarsal coalition is defined by abnormal fibrous, cartilaginous, or bony fusion of two or more tarsal bones. Bony coalition is characterized by the presence of a bony bar that extends between the involved bones. Complete fusion, when present, usually occurs by the age of 12. In the absence of a bony bar, fibrous and cartilaginous coalitions are usually evident by the presence of sclerosis and close approximation of the bones in question. Tarsal coalition is usually sporadic. Talocalcaneal tarsal coalition occurs as a result of failure of tarsal bone segmentation. Talonavicular coalition is uncommon and may be associated with a genetic hereditary transmission, either dominant or recessive; it has a described association with anomalies of the little finger. The association of coalition with other malformations suggests that the ball-and-socket ankle joint that can occur in patients with coalition results from a global developmental abnormality of the ankle and foot. At birth, the coalition is liable to be fibrous, with ossification occurring during the second decade of life. The resulting ankylosis leads to abnormal biomechanical forces, which may in turn cause the development of secondary osteoarthritis. The patient may be asymptomatic, and the abnormality may be discovered incidentally at the time of trauma or because of limitation of athletic interests. When symptomatic, the majority of coalitions may present with a painful flatfoot with associated peroneal spasm. On examination, subtalar movements are limited (inversion/eversion and anterior gliding). A tarsal tunnel syndrome may be present. Although calcaneonavicular coalition is the most common coalition, including all subtypes, that is, bony, cartilaginous, and fibrous, talocalcaneal coalition accounts for ~60% of bony coalitions and is thus seen more frequently on conventional radiographs. Quoted figures for the incidence of bilaterality vary dramatically from 20 to 80%. Occasionally, there is more than one type of coalition in the same foot.
Tarsal Coalition
Clinical Presentation


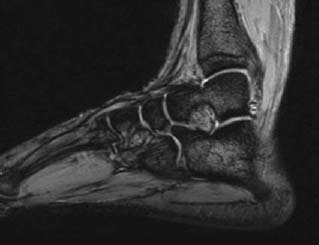
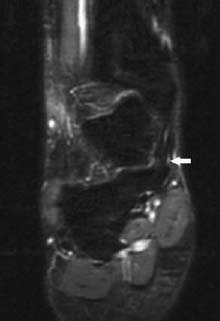
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Clinical Findings
TALOCALCANEAL COALITION
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


