35 Miscellaneous Osteoarthropathies
Aside from crystal-induced arthropathies, a number of other osteoarthropathies affect the bone structure and the joints. These include sarcoidosis, amyloidosis, sickle-cell anemia, thalassemia, and multicentric reticulohistiocytosis. The displacement of normal bone substance by granulomatous tissue, metabolic products, or abnormal erythropoiesis is reflected in characteristic radiographic features. Neurotrophic disorders causing carpal malalignment and, less often, hemophilia with recurrent hemorrhages, can lead to bizarre destruction of the wrist, which can be visualized in MRI with high sensitivity. Periosteal bone appositions can be the primary result of hypertrophic osteoarthropathy or can be caused by other, usually thoracic, diseases. Osteoarthropathies induced by ionized radiation are now very rare.
Sarcoidosis (Boeck Disease)
Pathoanatomy and Clinical Symptoms
This systemic disease of unclear etiology is manifested as skeletal sarcoidosis in 1–15% of cases. Noncaseating, epitheloid-cell granulomas infiltrate the synovial membranes and also the bone marrow. This leads to acute and chronic arthritis as a result of granulomatous synovitis, which must be differentiated from acute, unspecific concomitant arthritis. Sarcoidosis of the bone marrow leads directly to osseous defects with lytic lesions, as well as osteopenic and osteosclerotic lesions. The skin and lungs are affected in 80–90% of cases.
Diagnostic Imaging
Radiography
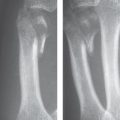
In the hand, skeletal sarcoidosis most often appears with a specific distribution pattern. The middle and distal phalanges of the fingers are predisposed sites; the proximal phalanges and metacarpals are less often affected ( Table 35.1 , Fig. 35.1 a, b). The distribution is unilateral or bilateral, but not strictly symmetrical.
Subperiosteal bone resorption, radial periosteal spicules, or soft-tissue calcifications are observed less often in sarcoidosis. The rare sarcoid dactylitis (0.2%), which causes cystic lesions in the cancellous bone and periosteal reactions, is accompanied by a painful, erythematous swelling of the phalangeal soft tissues (Fig. 35.1b, c), analogous to the sausage-shaped fingers in psoriatic arthritis. The osseous characteristic of lupuspernio is an aggressive, permeating bone destruction.
|
Nuclear Medicine
Skeletal scintigraphy with 99mTc phosphates documents the affected bone regions and the extent of damage with high sensitivity but unspecifically. Gallium-67 (67Ga) citrate scintigraphy also identifies sarcoid foci in the skin, internal organs, and muscles.
Magnetic Resonance Imaging
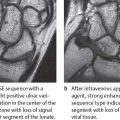
Noncaseating granulomas have low to middle signal intensity in T1-weighted sequences and high signal intensity in T2-weighted sequences. They show only moderate contrast enhancement (Fig. 35.1c).
Differential Diagnosis
Enchondromas, fibrous dysplasia, neoplastic osteolyses, uricate arthritis, rheumatoid arthritis, rheumatic fever, hyperparathyroidism, and childhood tuberculosis (spina ventosa) must be differentiated radiographically. Hilar adenopathy, altered pulmonary structure, and erythema nodosum are characteristics of sarcoidosis.
Therapeutic Options
Articular complaints can be treated well with nonsteroidal anti-inflammatory agents (NSAIDs); glucocorticoids are rarely necessary. Orthopedic surgery can be required for extremely rare cases with joint destruction.

Neurogenic Osteoarthropathy and Charcot Osteoarthropathy
Pathoanatomy and Clinical Symptoms
Hypertrophic or atrophic Charcot osteoarthropathy is caused by diseases of the central nervous system, especially of the spinal cord and of peripheral nerves. The underlying pathophysiology is reduced sensoric perception and proprioception, and muscular hypotonia but retained movement. This leads to instability, biomechanical overload of the joints, and, finally, to intraarticular fractures. Disturbances of vegetative innervation and vasomotor reflexes are thought to be responsible for the trophic bone fragility and active bone resorption. The most common primary diseases include tabes dorsales (80%), especially affecting the lower extremities, syringomyelia (10%) affecting the upper extremities (glenohumeral joint, elbow, and wrist) in 80% of cases, occasionally diabetes mellitus, and, rarely, multiple sclerosis. Diabetic osteoarthropathy is classically manifested in the talonavicular and tarsometatarsal joints. The diabetic hand has flexion contractures of the finger joints, while carpal and phalangeal osteoarthropathy is rare. Neural leprosy causes peripheral nerve lesions followed by atrophy of the hand and foot skeleton.
Diagnostic Imaging
The characteristic feature is “anarchistic remodeling and disintegration” (Dihlmann) of the joints that far exceeds that of normal osteoarthritis and other arthritic diseases ( Table 35.2 , Fig. 35.2 ).
Differential Diagnosis
Only in the early stages of neurogenic arthropathy, osteoarthritis, crystal-induced osteoarthropathies, and osteonecrosis should be considered as differential diagnoses. However, the characteristic presentation usually indicates Charcot disease.
Therapeutic Options
The lax joints are stabilized with orthopedic devices to retain the greatest possible degree of function. If neurogenic osteoarthropathy is diagnosed early enough, synovectomy leads to good results. Arthrodesis and alloarthroplasty are unfavorable because of the common occurrence of nonunion and secondary wound healing.
|
Peculiarities on the hand
|

Hemophilic Osteoarthropathy (“Bleeder’ Joints”)
Pathoanatomy and Clinical Symptoms
Coagulopathic osteoarthropathy is most often associated with X-chromosomal recessive hemophilia A (deficiency of coagulation factor VIII) and hemophilia B (deficiency of factor IX), rarely with hemophilia C (factor XI deficiency), and with inherited hypoproconvertinemia (factor VII deficiency). Individual cases have been observed with coumarin treatment, liver diseases, and thrombocytopathies. When a coagulation factor has less than 1% of its normal activity, this always leads to severe, even spontaneous intraarticular hemorrhages. In childhood, bleeders’ joints are most often seen in the upper ankle, the elbow, and the knee joints. The pathogenesis of the arthropathy in the large and small joints is analogous. Just a few recurrent hemorrhages into the joint cavity will lead to destruction of the articular cartilage and successive destruction of the synovium and the joint capsule. An intra-articular increase in pressure triggers epiphyseal and apophyseal growth disturbance, bone disintegration, and pressure erosions of the areas not protected by cartilage. Chronic arthropathy can end in fibrous or even osseous ankylosis. Hemophilic pseudotumors develop after repeated subperiosteal and intraosseous hemorrhages, which induce alternating bone resorption and bone formation. The osteopathic lesions often lead to pathologic fractures.
Diagnostic Imaging
Radiography
The joints of the hand are involved in 5–14% of hemophilic arthropathy; the metacarpophalangeal joints are most affected (40%). The proximal interphalangeal (5%) and carpal joints (3%) are affected far less often ( Table 35.3 ).
Magnetic Resonance Imaging
Early signs that are decisive for therapy can be visualized in MR imaging. If the radiograph is normal, MRI is the most sensitive procedure for identifying degraded blood products in hemophilic joints. In the subacute stage of hemorrhage, methemoglobin appears hyperintense in both T1- and T2-weighted sequences. After recurrent hemorrhages, paramagnetic hemosiderin is hypointense in signal, particularly in GRE sequences, and causes a decrease in signal intensity in the otherwise hyperintense, hypertrophed synovium in T2-weighted sequences. Even incipient cartilaginous thinning can be visualized in large joints.
Differential Diagnosis
Hemoglobinopathies and acquired coagulopathies must be clarified, and traumatic sequela, osteonecrosis, and infections can be excluded. A hemophilic pseudotumor must be differentiated from a Ewing sarcoma and osteomyelitis.
Therapeutic Options
Substitution of the affected coagulation factor is the foundation of prophylaxis and treatment of joint hemorrhages. If the hemorrhagic joint effusion is not rapidly resorbed, puncture or arthroscopic lavage should be considered. Synoviorthesis can be performed for synovitis, which has become rare. The indication for corrective osteotomy and joint replacement can, in close cooperation with experienced hematologists, be decided upon just as in nonhemophilic patients.
Hemophilic arthropathy
|
Hemophilic pseudotumor
|
Amyloid Osteoarthropathy
Pathoanatomy and Clinical Symptoms
Amyloid is an inhomogeneous substance consisting of amino acids of different origins and composition that has an affinity for Congo red dye and forms either generalized or focal extracellular deposits in different organs. Aside from idiopathic and inherited amyloidoses, the associated generalized forms are the most common. These can be found in patients with chronic infections, rheumatic inflammations, collagenoses, ulcerative colitis, malignomas (amyloid A), multiple myeloma, and Waldenström disease (amyloid L), and in patients undergoing dialysis (amyloid B = β2-microglobulin). Focal amyloidoses are known to occur with type II diabetes mellitus (amyloid E) and in senility (senile amyloidosis, a yloid S), but their role in these diseases is not known. Arthropathy develops in 5–13% of cases, particularly idiopathic and paraproteinemic and hemodialysis-associated amyloidosis. Amyloid deposits in cartilage, the synovium, the capsuloligamentary system, the joint cavity, and bones lead to stiffness and limited range of motion. The above must be differentiated from polyneuropathic arthropathy in hereditary amyloidoses and monoclonal gammopathies.
|

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


