41 Computed Tomography Artifacts
41.1 Computed Tomography Angiography
41.1.1 Case Presentation: CTA Artifacts Mimicking Carotid Artery Dissection
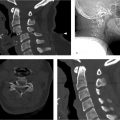
History: A 35-year-old man admitted to the neurosurgical service for management of a subdural hematoma suffered during motor vehicle collision. A CT angiography (CTA) of the neck was performed as routine screening based on the mechanism of the injury ▶ Fig. 41.1. The radiology report describes a dissection of the left carotid artery origin (see ▶ Table 41.1).

Imaging impression: Normal carotid bifurcation; the apparent filling defect is artifactual.
Cause: Artifactual hypodensity secondary to turbulence related to the carotid bifurcation, resulting in heterogeneous mixture of contrast and nonopacified blood.
Additional testing to consider in difficult cases:
Recommended: Delayed contrast examination, such as routine contrast-enhanced CT of the neck. This admixture phenomenon is extremely transient and relates to the high speed of modern multidetector scanners.
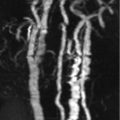
Not recommended: Two-dimensional time-of-flight MR angiography. If there is turbulence at the bulb significant enough to produce this artifact on CT, it will almost certainly produce a similar artifact on MRI, although the physics is completely different.
Other common phenomenon that may simulate acute dissection on CTA:
CT beam hardening artifact: Streaklike artifact related to high-density material such as dental amalgam or other radiopaque foreign bodies as well as high-density contrast in the venous system. The resulting hypodense linear bands projected from the dense object traverse the vessel in the axial plane, resulting in linear filling defects on the reconstructed images, and sometimes a flaplike appearance may be present even on the source images.
Pulsation artifact: Motion of the carotid artery during the CT acquisition results in the superimposition of the carotid density on adjacent structures, resulting in a Venn diagram type of overlap appearance on the axial image. This can then result in irregularity in the contour of the vessel lumen or the appearance of linear flaplike filling defects on reconstructed images. This primarily occurs in in two locations: at the thoracic junction, where the carotid artery pulsatility is more marked, and, in children and younger patients, in the internal carotid artery where it lies immediately adjacent to the internal jugular vein.
FMD: Thickening of the vessel wall can result in a beaded, irregular appearance very similar to arterial dissection. Often bilateral, it can involve the vertebral arteries as well. It is important to recognize that FMD is associated with intracranial aneurysms and real dissections.
41.1.2 Companion Cases
Companion Case 1

Companion Case 2

Companion Case 3

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


