CASE 42 George Nomikos, Anthony G. Ryan, Peter L. Munk, and Mark Murphey A 53-year-old man presented with pain in the proximal humerus for 3 months. Figure 42A Figure 42B Figure 42C Figure 42D A radiograph (Fig. 42A) shows a lytic destructive lesion in the proximal femur. There is associated cortical thickening and periosteal reaction, as well as expansile remodeling and lobular endosteal scalloping. The density in the greater trochanter represents a methylmethacrylate plug from a prior biopsy. The CT (Fig. 42B) shows cortical destruction, faint internal mineralization, and soft-tissue thickening around the femur. The sagittal inversion recovery MRI (Fig. 42C) shows the extent of the lesion. The lesion is predominantly high signal intensity. The lower signal intensity foci within the lesion represent areas of mineralization. The postcontrast image (Fig. 42D) shows peripheral and septal enhancement, a characteristic pattern seen in hyaline cartilage lesions. There is also enhancement within the periosteal reaction around the femur. Chondrosarcoma. Chondrosarcomas account for ~8 to 17% of biopsied primary bone tumors. They may arise in the medullary canal (central type) or on the surface of the bone (peripheral type). Chondrosarcomas represent malignant cartilage lesions. They may arise de novo or from a preexisting cartilage lesion, such as an enchondroma or osteochondroma. Common locations include the pelvis, femur, humerus, ribs, tibia, scapula, and spine.
Chondrosarcoma
Clinical Presentation

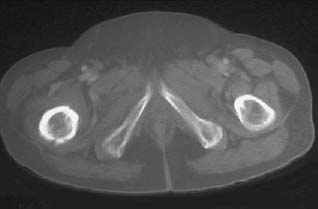

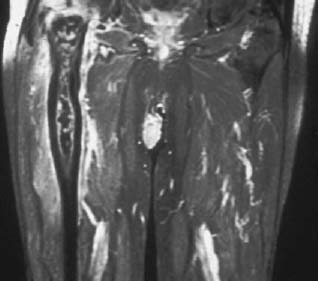
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


