42 Infections of the Soft Tissues
Soft-tissue infections in the hand comprise paronychia, felons, pyogenic tenosynovitis, deep space infections of the palm, gangrenous infections, and acute calcium hydroxyapatite deposits. The diagnosis is usually made clinically. Skeletal scintigraphy allows early exclusion of concomitant osteomyelitis. Only soft-tissue calcifications and air inclusions can be identified in survey radiographs. High-resolution ultrasonography (US) is the method of first choice to identify and estimate the extent of an infection. MRI should be applied if an abscess in the deep spaces of the palm is suspected or if there is spread into multiple compartments.
Pathoanatomy and Clinical Symptoms
Infections of the soft tissues of the hand comprise a heterogeneous group of diseases. A common cause of infection is a penetrating injury through which pathogenic organisms are inoculated into the soft tissues. Even the tiniest injuries are sufficient, such as tears in the paronychial tissue occurring during nail care. Since there are a number of anatomically demarcated, enclosed compartments in the hand, infections usually remain at their primary site of origin in initial stages; this includes the subcutaneous or deep spaces in the palm, the tendon sheaths, and the joints. Patients with a compromised immune system and/or sensory deficiency (as in diabetes mellitus and severe carpal tunnel syndrome) are predisposed to infection. The clinical symptoms include the classic signs of inflammation (redness, hyperthermia, swelling, pain, and functional impairment), though they cannot always be recognized in their full extent. The findings from the physical examination are often sufficient to make the final diagnosis.
Diagnostic Imaging
Radiography
Radiographic survey views in two planes, in low-kilovoltage radiography if necessary, can provide evidence of inflammatory involvement of the bony skeleton of the hand, e.g., phalangeal osteomyelitis or infectious arthritis. Soft-tissue calcifications are seen in acute calcium (hydroxyapatite) deposition, chondrocalcinosis (calcium pyrophosphate dihydrate deposition), and sometimes in tuberculosis of the tendon sheath.
Nuclear Medicine
Three-phase scintigraphy is well suited to confirm or exclude osseous involvement with the uptake of osteotrophic radioactive pharmaceuticals. Soft-tissue infections lead to regional hyperemia, which results in increased bone metabolism in the affected area. The resulting ratios usually do not exceed 3.0, as shown in animal experiments. Furthermore, increased nuclide uptake is rather diffusely distributed. If the bone is involved as a result of soft-tissue infections (periostitis, osteitis, osteomyelitis), circumscribed parts of the skeleton show a marked increase in nuclide uptake, indicating new bone formation, in the 24-hour scintigram.
Ultrasonography
High-resolution US is the method of choice in clinically unclear inflammatory conditions. Only probes of 10 MHz or more should be used. These can reliably determine whether an inflammatory process is already transformed into colliquation, i.e., an abscess. A further important indication is the search for infectious foreign bodies that cannot be seen in radiographs.
Computed Tomography
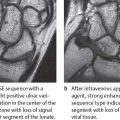
CT is only rarely applied in the evaluation of soft-tissue inflammation. Intravenous administration of a contrast agent is an essential prerequisite for diagnosis of abscesses. A few minutes after contrast application, a ring-shaped enhancement in the periphery of an abscess appears without enhancement in the center. For the hand, axial slices using the spiral CT technique and image calculation with a soft-tissue kernel are recommended.
Magnetic Resonance Imaging
MRI is the procedure offering the greatest diagnostic relevance in inflammatory processes in the soft tissues of the hand. Prerequisites for hand MRI are a high-resolution technique and venous administration of gadolinium. Axial slices with T2-weighted FSE sequences and contrast-enhanced T1-weighted SE sequences are most suitable to identify inflammation of the compartments of the deep spaces in the hand. The other spatial planes determine the extent of the inflammatory process in proximal and distal directions. The signal intensity and pattern of contrast enhancement differentiate between cellulitis and an abscess, a distinction that is essential for terapeutic decision.
Disease Entities
Infections of the Fingertips and Paronychia
Pathoanatomy and Clinical Symptoms
These involve inflammation of the cutaneous and subcutaneous tissues. The condition often follows a minimal injury, e.g., paronychia as an inflammation of the nail wall caused by a skin lesion occasioned in cutting the fingernails.
Radiography
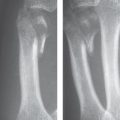
Radiographs that are centered on the clinical maximum of the infectious process can locate nonradiolucent foreign bodies that initially triggered the infection. They are also necessary to confirm or exclude the presence of osteomyelitis or infectious arthritis ( Fig. 42.1 ). Table 42.1 summarizes the radiographic criteria.
|

Pyogenic Flexor Tenosynovitis
Pathoanatomy and Clinical Symptoms
Pyogenic tenosynovitis is caused by pathogens that either directly enter the circular tendon sheaths in the metacarpal area or fingers (penetrating injuries) or spread from subcutaneous abscesses. During clinical examination, there is pressure pain above the site of injury and pain over the proximal portion of the flexor-tendon sheath when pressure is placed on the palm. The often-described V-shaped phlegmon is rarely involved according to our personal experience, but we have observed phlegmons that have spread proximally from the thumb through the carpal canal. This appears clinically as a highly acute carpal tunnel syndrome resulting from compression of the median nerve.
Diagnostic Imaging
Radiography
Radiographs serve to exclude concomitant osteomyelitis and/or arthritis and to detect foreign bodies.
Ultrasonography
A focal or diffuse synovial thickening can be demonstrated ( Fig. 42.2 ). The inflamed and thickened tendon sheath displays moderate echos and is neighbored by hypoechoic synovial fluid. This constellation is always pathologic in flexor tendons. Enclosed foreign bodies can be detected by means of dense echoes and distal acoustic shadow. They are usually found in the center of the infection.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


