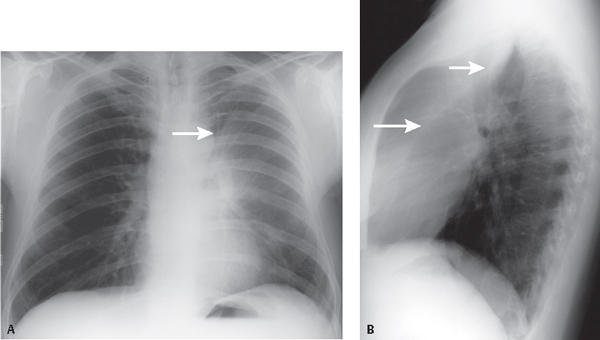
CASE 42 42-year-old man with complaints of cough, fever, and shortness of breath PA (Fig. 42.1A) chest radiograph shows an ill-defined left perihilar and upper lobe opacity without perceptible air bronchograms that partially silhouettes the upper left heart border. The left thorax appears smaller than the right. The left diaphragm is elevated. A hyperlucent crescent (arrow) insinuates between the perihilar opacity and the transverse aorta and outlines the aortic arch. The lateral exam (Fig. 42.1B) demonstrates a retrosternal sigmoid band of increased opacity and marked anterior displacement of the oblique fissure (arrows). Left Upper Lobe Atelectasis; Endobronchial Carcinoid Tumor • Uncomplicated Upper Lobe Atelectasis (e.g., obstructing mucus plug, foreign body) • Complicated Upper Lobe Atelectasis Fig. 42.1 The major difference between atelectasis of the left and right upper lobes is the absence of a horizontal fissure in the left thorax. Thus, all lung tissue anterior to the oblique fissure is involved. On lateral chest radiography, the oblique fissure shifts forward in a plane roughly parallel to the anterior chest wall (Fig. 42.2). As volume loss increases, the fissure moves further anteriorly and medially, until the opacity of the collapsed lobe is no more than a broad linear opacity contiguous and parallel to the anterior chest wall (Figs. 42.1B, 42.2, 42.3B). On frontal chest radiography, contiguity of the atelectatic upper lobe with the anterior mediastinum obliterates the upper left cardiac border (silhouette sign) (Figs. 42.1A, 42.2, 42.3A). As the apical segment collapses, the space it vacates becomes “filled in” by compensatory overinflation of the left lower lobe superior segment. The apex of the thorax will contain aerated lung which can mimic an apical pneumothorax. The over-inflated superior segment may also insinuate between the collapsed upper lobe and mediastinum, sharply delineating the aortic arch by a hyperlucent air crescent (Luftsichel sign) (Figs. 42.1A, 42.3A). On CT, the atelectatic upper lobe will abut the anterior chest wall and mediastinum (Figs. 42.3C, 42.3D, 42.3E, 42.3F). The oblique fissure will be displaced cephalad and anteriorly (Figs. 42.3C, 42.3D
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Endobronchial Mass (e.g., primary and secondary neoplasia)
Endobronchial Mass (e.g., primary and secondary neoplasia)
 Extrinsic Bronchial Compression by Reactive or Neoplastic Lymphadenopathy
Extrinsic Bronchial Compression by Reactive or Neoplastic Lymphadenopathy
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


