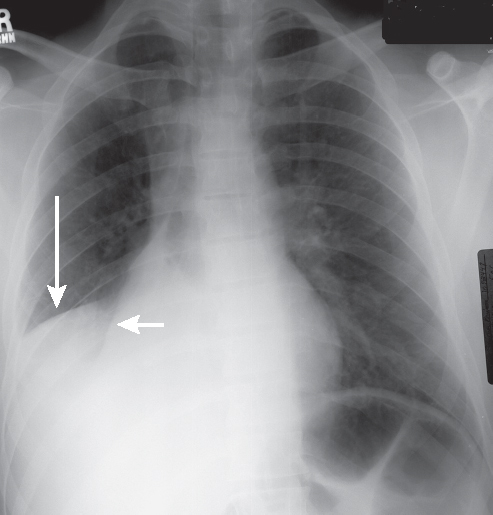
CASE 44 42-year-old man with an acute asthma exacerbation, chest pain, and shortness of breath PA (Fig. 44.1) chest radiograph shows inferior displacement of the oblique (short arrow) and horizontal fissures (long arrow). A radio-opacity silhouettes both the right heart border and the right diaphragm. This opacity extends to but does not blunt the lateral sulcus. Note the discrepancy in volume between the right and left thorax and the rightward mediastinal shift. Combined Right Middle and Lower Lobe Atelectasis; Mucus Plug Bronchus Intermedius • Isolated Right Lower Lobe Atelectasis • Right Subpulmonic Pleural Effusion • Large Right Pleural Effusion Fig. 44.1 Simultaneous right middle and lower lobe collapse localizes the obstructing lesion to the bronchus intermedius. This combination of bilobar atelectasis may be misinterpreted as isolated right lower lobe collapse on frontal chest exams and as subpulmonic effusion on lateral X-rays. Extension of the increased opacity to the lateral costophrenic angle on the frontal exam supports the diagnosis of bilobar collapse. On lateral chest exams, the upper border of a subpulmonic effusion is usually flat superiorly and appears to terminate at the oblique fissure anteriorly (“rock of Gibraltar” sign) (see Section XII, Case 171). Alternatively, the opacity created by bilobar atelectasis extends from the front to the back of the chest (Fig. 44.2). Affected patients may exhibit an abrupt drop in oxygen saturations, altered A-a gradient, and diminished breath sounds over the affected region. • Frontal radiography
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Clinical Findings
Imaging Findings
Radiography
 Silhouette of right atrial border (atelectatic middle lobe) (Figs. 44.1, 44.3)
Silhouette of right atrial border (atelectatic middle lobe) (Figs. 44.1, 44.3)
 Silhouette of right hemidiaphragm (atelectatic lower lobe) (Figs. 44.1, 44.3)
Silhouette of right hemidiaphragm (atelectatic lower lobe) (Figs. 44.1, 44.3)
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


