CASE 63 George Nomikos, Anthony G. Ryan, Peter L. Munk, and Mark Murphey A skeletally immature male presented with a knee pain complaint. Figure 63A Figure 63B Figure 63C Radiologic work-up shows a lytic lesion in the proximal tibial epiphysis that has a narrow zone of transition with a mild rim of surrounding sclerosis (Fig. 63A). The lesion does not cross the physis. There is faint punctate mineralization in the lesion, better seen on the CT scan (Fig. 63B), with an appearance of chondroid matrix. There is also marked cortical thinning caused by the lesion posteriorly. There is no evidence of cortical penetration. CT scan obtained through the tibia more distally (Fig. 63C) shows smooth, thick, nonaggressive periosteal reaction along the tibial shaft distal to the lesion. Chondroblastoma. Chondroblastoma is an uncommon benign primary neoplasm of bone, accounting for ~1% of all primary bone tumors. Most lesions arise in the epiphysis or apophysis of long tubular bones. The knee accounts for ~30 to 40% of cases. The femur is the most commonly involved bone (33% of all cases and equally divided between proximal and distal locations), followed by the humerus and tibia. The talus and calcaneus are common sites of involvement in the hindfoot. Equivalent epiphyseal and apophyseal locations such as the patella and greater trochanter of the femur are not uncommon. Isolated metaphyseal involvement is uncommon (10% in our experience). The hands and feet account for 10% of lesions. Although the reported age range is broad, most patients are in their second decade of life at the time of diagnosis, and 90% of all lesions occur in patients between 5 and 25 years of age. Chondroblastoma is 1.4 to 2.0 times more common in men than in women. The most common presenting symptoms are pain, swelling, and limited range of motion. Muscle wasting may also be seen.
Chondroblastoma
Clinical Presentation

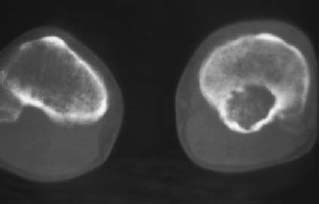
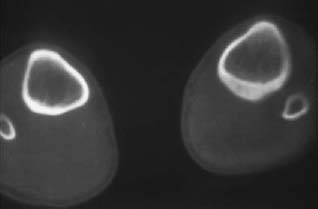
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Clinical Findings
Pathology
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


