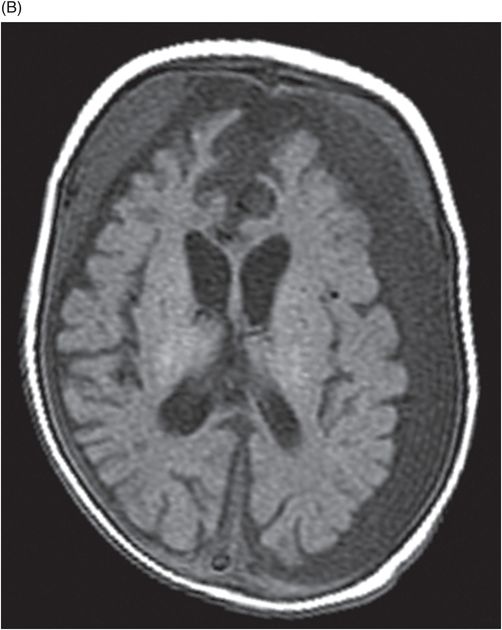
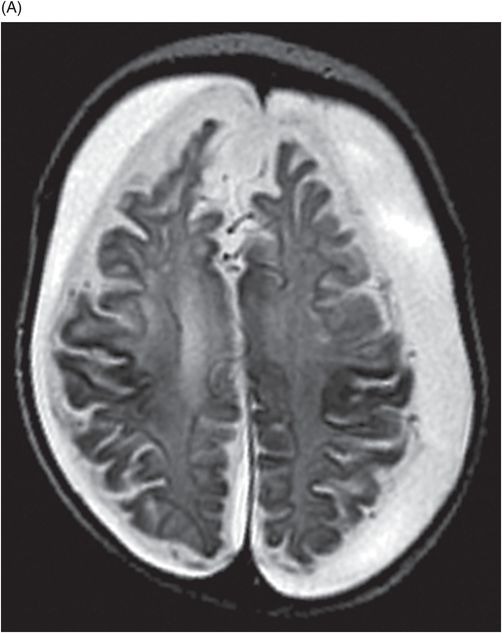
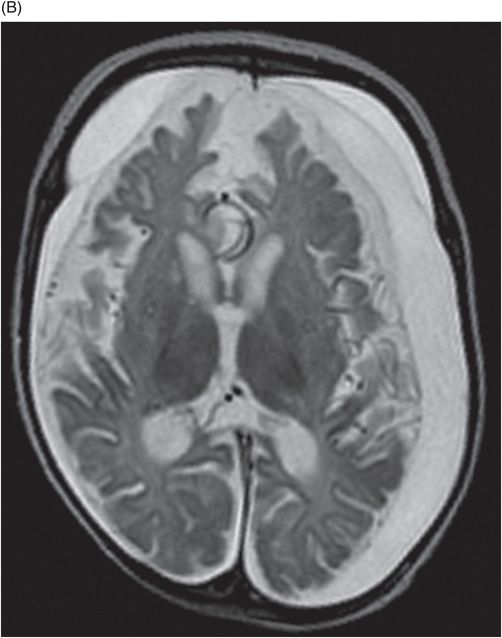
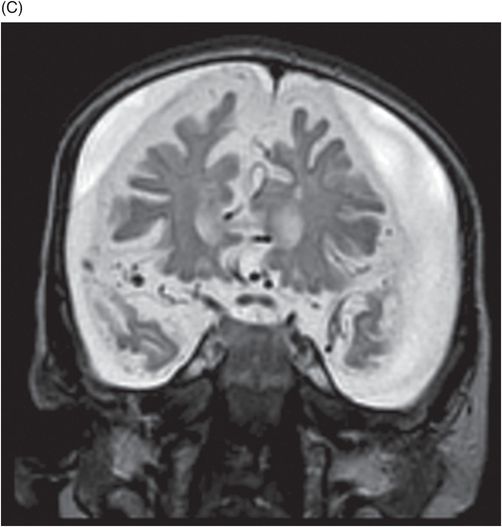
(A) Axial T2WI of the brain at the level of corona radiata. (B) Axial T2WI of the brain at the level of lateral ventricles. (C) Coronal T2WI at the level of frontal horns and anterior temporal lobes.

Menkes Disease
Primary Diagnosis
Menkes disease
Differential Diagnoses
Non-accidental trauma
Glutaric aciduria type 1
Leigh disease (subacute necrotizing encephalopathy)
Phenylketonuria
Imaging Findings
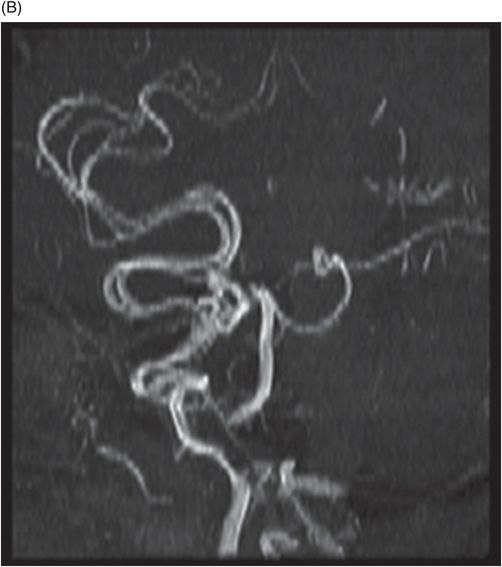
Fig. 67.1: (A) Axial T1WI of the brain at the level of corona radiata and (B) Axial T1WI at the level of lateral ventricles demonstrated bilateral subdural collections with varying stages of hemorrhage along the cerebral convexities. Fig. 67.2: Axial T2W images (A) and (B) at the same levels as those in Fig. 67.1 and (C) at the level of anterior temporal lobes and frontal horns demonstrates generalized cerebral atrophy and white matter changes. Fig. 67.3: (A–B) Magnetic resonance angiography demonstrates tortuous intracranial vasculature.
Discussion
The most important differential consideration in an infant presenting with failure to thrive and suspicious cranial imaging is child abuse, which can mimic Menkes disease. The combination of calvarial fractures on X-rays with subdural hygromas and hematomas of varying ages, coupled with bone fractures favors abuse. Clinical correlation with skin and hair abnormalities, serum copper levels, and tortuous intracranial vessels on MRI favor Menkes disease.
Glutaric aciduria type 1 is an inborn autosomal recessive metabolic disorder resulting from deficiency of glutaryl-CoA dehydrogenase. Clinically it presents with macrocephaly, seizures, dystonia, encephalopathy, and developmental delay. On MR imaging, widening of the sylvian fissures is the most noted, characteristic feature in confirmed cases. Other findings include signal abnormalities involving the basal ganglia, dentate nuclei, and frontotemporal atrophy. Subdural hygromas can also occur in patients with glutaric aciduria, which can mimic Menkes disease, but can be differentiated by other MR imaging findings. Differential diagnoses also include Leigh disease and phenylketonuria: Unusual pathologies with associated signal abnormalities on diffusion imaging that mimic mitochondrial disease have been described in the literature. However, serum copper and ceruloplasmin concentrations would be normal in other metabolic disorders presenting with cutaneous manifestations, macrocephaly, and other neurologic symptoms, whereas they are low in Menkes disease.
Menkes disease, also known as trichothiodystrophy or kinky hair syndrome, is a rare, X-linked recessive, lethal neurodegenerative disorder of impaired copper transport. It is estimated to occur in 1/300,000 people. Initial presentation during the first few months of life is non-specific and may include lethargy, hypotonia, cephalohematomas, jaundice, and hypoglycemia. As the condition progresses, patients develop the characteristic, short, coarse, wiry hair, often by four to five months of age. This is accompanied by progressive neurologic deterioration. Seizures, failure to thrive, loose skin, pectus excavatum, urinary bladder diverticula, retinal hemorrhages, and developmental delay occurring by one year of age can also be seen. Menkes disease is usually lethal by two or three years of age, with respiratory failure cited to be the most common cause of death.
The X-linked recessive disorder is caused by a mutation in the ATP7A gene, located on chromosome Xq21.1, which results in abnormal functioning of the copper-dependent enzyme adenosine triphosphate, thus leading to dysfunctional cellular transport and metabolism of copper, causing lower serum levels of copper.
At birth, neuroimaging is often normal. As the disease progresses, symmetric cerebral and cerebellar volume loss occurs, often in association with bilateral subdural collections, both apparent on CT and MRI. Magnetic resonance imaging T1-weighted images can show hyperintense signal in the basal ganglia, similar to that of chronic hepatic encephalopathy. Magnetic resonance angiography reveals tortuous, elongated vessels. As the diagnosis is not often clear, skeletal radiographs are typically obtained, which show long bone osteoporosis, metaphyseal spurring, periosteal reaction, and scalloping of the vertebral bodies posteriorly.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


