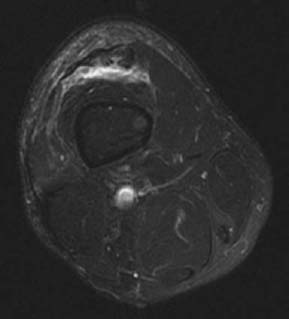
CASE 7 Anthony G. Ryan and Peter L. Munk A 26-year-old insulin-dependent patient with diabetes sustained a combined extension against resistance and direct impact injury as a result of a heavy tackle while playing amateur soccer. He complained of immediate excruciating pain in his distal thigh and had almost complete loss of active knee extension on examination. Figure 7A Figure 7B Figure 7C Figure 7D Figure 7F Sagittal T2 (Figs. 7A, 7B), sagittal T1 (Fig. 7C), axial proton density fat-saturated (Figs. 7D,7E), and coronal T2 (Fig. 7F) images show focal discontinuity, thickening, and signal heterogeneity within the proximal quadriceps tendon at the level of the musculotendinous condensation. Fluid signal intensity is evident on the T2 images anterior and posterior to the tendon. High signal intensity is also evident within the substance of the adjacent muscles of the anterior compartment: rectus femoris, vastus intermedius, vastus medialis, and vastus lateralis. Quadriceps tendon tear. None. The extensor mechanism of the knee joint consists of the quadriceps muscle and tendon, patella, patellar tendon, and patellar retinacula. The quadriceps tendon itself is a conjoint tendon of the four muscles of the anterior compartment of the thigh—the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius—which are the major extensors, and consequently stabilizers, of the knee joint. Rupture of the quadriceps tendon is uncommon in the absence of conditions predisposing to tendinopathy. The tendon may be weakened because of chronic degeneration or inflammation, which may then produce an exercise-related rupture secondary to less forceful contraction. Endogenous disorders giving rise to tendon weakness include diabetes mellitus, rheumatoid arthritis, and seronegative spondyloarthropathy. Primary and secondary hyperparathyroidism: End-stage renal disease is frequently associated with distal quadriceps rupture, secondary to a combination of the secondary hyperparathyroidism and subtendinous bone resorption. Exogenous factors predisposing to tendinopathy include mechanical impingement, repetitive overuse, systemic steroid use or abuse, and repeated intra-articular or bursal injection of steroids. As many as 50% of patients with closed femoral shaft fractures have accompanying injuries of the extensor mechanism (Fig. 7G). Contusions to the muscle belly are usually sustained by direct trauma secondary to contact sport activities or motor vehicle collisions. Strain of the complex is most likely to happen at the musculotendinous junction. Rupture of the distal quadriceps secondary to end-stage renal disease occurs as a result of the combination of secondary hyperparathyroidism and subtendinous bone resorption. Acute injuries are associated with edema, hemorrhage, and fluid collections. Complete disruption of the extensor mechanism may be associated with osseous avulsion of the superior pole of the patella (Figs. 7H,7I). Figure 7G Lateral radiograph of the knee after fixation of distal femoral and proximal tibial fractures. Calcifications are evident in both quadriceps and patellar tendons, indicative of the combined injury sustained at the time of the initial insult.
Quadriceps Mechanism Tear
Clinical Presentation
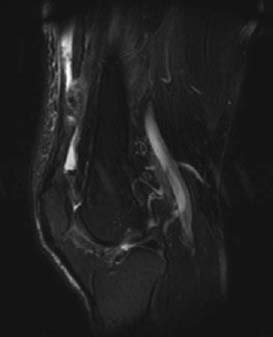
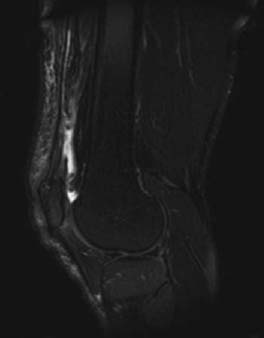
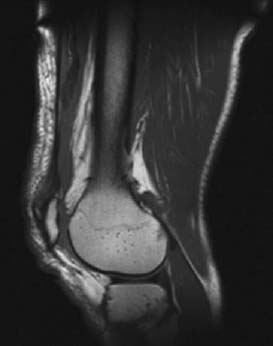
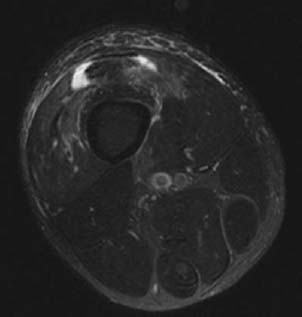
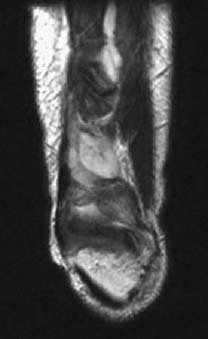
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


