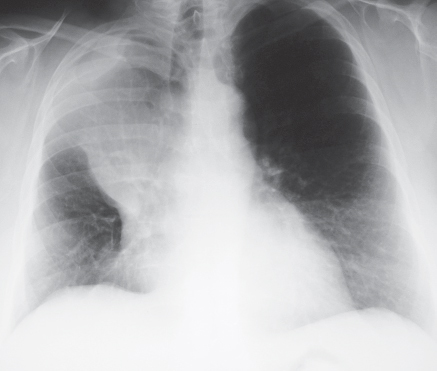
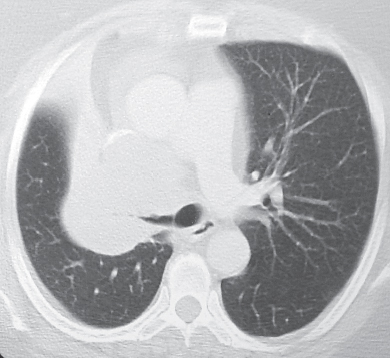
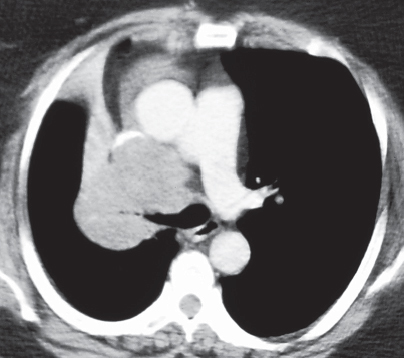
CASE 76 57-year-old woman with cough, hemoptysis and weight loss PA (Fig. 76.1) and lateral (Fig. 76.2) chest radiographs demonstrate a large right hilar mass with associated upper lobe volume loss. Note the reverse “S” shape produced by the concave outline of the lateral aspect of the minor fissure and the convex outline of the central mass (Fig. 76.1), the so-called reverse “S” sign of Golden. Contrast-enhanced chest CT (lung and mediastinal windows) (Figs. 76.3, 76.4) reveals a large central mass that produces severe irregular narrowing of the right mainstem bronchus (Fig. 76.3), atelectasis of the right upper lobe (Fig. 76.4), and deformity of the superior vena cava consistent with local invasion (Fig. 76.4). Lung Cancer; Squamous Cell Carcinoma • Lung Cancer, Other Cell Type • Other Primary Malignant Neoplasm • Lymphoma • Metastatic Disease Fig. 76.1 Fig. 76.2 Fig. 76.3 Fig. 76.4 Squamous cell carcinoma accounts for approximately 30% of all lung carcinomas. It is a malignant epithelial neoplasm characterized by microscopic keratinization and/or intercellular bridges. It exhibits rapid local growth and relatively late distant metastases. Squamous cell carcinoma has a strong association with cigarette smoking (over 90% affect smokers) and exposure to inhaled carcinogens, particularly arsenic. Squamous dysplasia and squamous carcinoma in situ are precursor lesions.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis

 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


