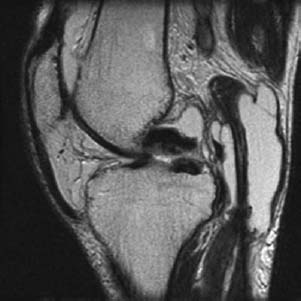
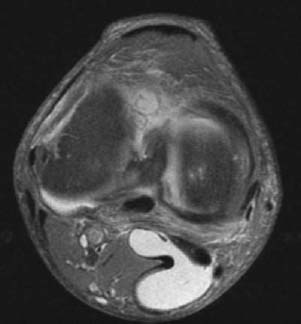
CASE 8 Anthony G. Ryan and Peter L. Munk A 54-year-old man presented with a painful mass posterior to the knee. Figure 8A Figure 8B Figure 8C Sagittal T2 MRI (Figs. 8A, 8B) and axial proton density fat-saturated images (Fig. 8C) show a lobulated high-signal intensity lesion communicating with a knee joint effusion via the interval between the tendons of the medial head of gastrocnemius and semimembranosus muscles. Popliteal (Baker’s) cyst. Although the appearances are typical of a popliteal cyst, in the appropriate circumstances, a popliteal artery aneurysm should be excluded. When a cyst is seen around the knee, the primary differential is between a meniscal cyst, tibiofibular cyst, cruciate cyst ganglion, and synovial cyst. A meniscal tear is typically found in the presence of a meniscal cyst. The proximal tibiofibular joint communicates with the knee joint in up to 10% of cases. If the mass is a cruciate cyst, its typical relationship to the anterior or posterior cruciate ligament should be clearly evident. Commonly found in patients with rheumatoid arthritis (60%) and less frequently found in non-rheumatoid patients, popliteal cysts are synovial cysts that communicate with the knee joint, unless the intervening channel is blocked secondary to recurrent inflammation. Popliteal cysts occur most frequently in the gastrocnemius-semimembranosus bursa, found, as its name suggests, between the tendons of the medial head of the gastrocnemius and the distal semimembranosus tendon. The larger the cyst, the more likely it will extend into unusual locations. Inferior and medial extension is relatively common, whereas lateral or cephalad extension is rare. The supralateral bursa may fill between the lateral head of the gastrocnemius and the distal end of the biceps, although this is uncommon, as is filling of the popliteal bursa, found beneath the lateral meniscus and anterior to the popliteus, where it may be confused for a meniscal cyst. If arthrography is performed, communication with the bursa is expected unless the channel is blocked, as above. The cysts may form different morphologies. For example, if intact, a cyst will be expected to have a smooth, well-defined contour. Most cysts are unilocular, although multiloculated cysts are not uncommon (Figs. 8D–8F). As the cyst enlarges, it may dissect along fascial planes (usually between the gastrocnemius and the soleus). If the cyst has ruptured, then a defined structure will not be seen; however, increased edema within the tissues of the calf will be demonstrated.
Popliteal Cyst
Clinical Presentation

Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


