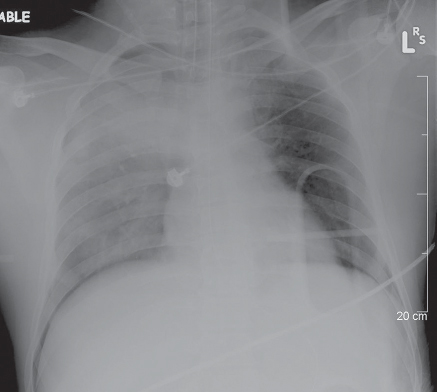
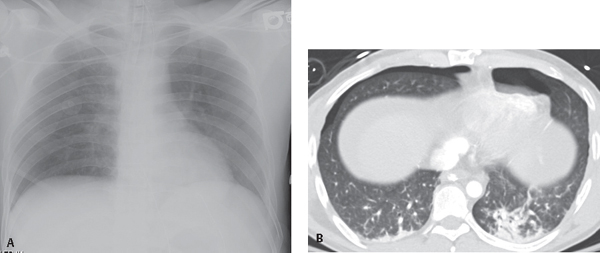
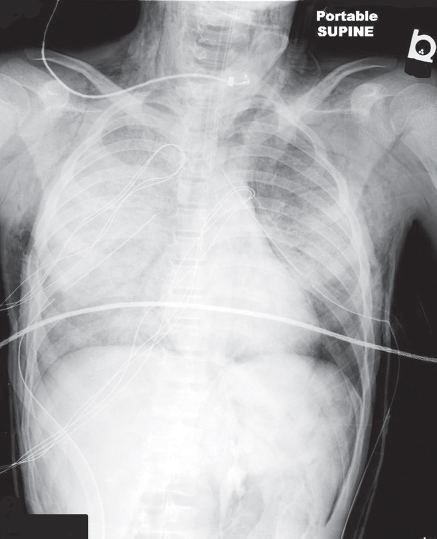
CASE 84 20-year-old man involved in a motorcycle collision with complicating head trauma and diminished breath sounds over the right thorax AP chest exam (Fig. 84.1) reveals right upper lobe consolidation and right lower lobe ground glass opacities consistent with pulmonary contusions. The right hemidiaphragm and ipsilateral costophrenic sulcus appear more pronounced, crisp, and hyperlucent than the left counterpart. Note the underlying backboard. Right Pneumothorax; Deep Sulcus Sign None Pneumothorax is a frequent complication after blunt or penetrating chest trauma. In blunt trauma, it is the second most common injury after rib fractures, occurring in 30–40% of patients. Occult pneumothorax, defined as a pneumothorax on chest or abdominal CT but not evident on chest radiography, is found in 2–12% of blunt trauma victims (Figs. 84.2A, 84.2B). Although many pneumothoraces are often initially small in volume, diagnosis is important, as an unsuspected pneumothorax may rapidly enlarge and become symptomatic in patients receiving mechanical ventilation. In the supine trauma patient, pleural air may preferentially accumulate in several recesses (also see Case 174). The anteromedial recess accumulates air first and accounts for up to 30% of pneumothoraces, but the problem is unrecognized on frontal supine chest exams in 30–50% of trauma patients. Left unrecognized and untreated, such pneumothoraces progress to tension in one-third of patients. Radiographic features of an anterior medial pneumothorax include the deep sulcus sign (Figs. 84.1, 84.3), manifest by a deep lucent costophrenic sulcus. Tension pneumothorax is an emergent clinical and not a radiologic condition that should be diagnosed and treated before the acquisition of imaging studies. However, unexpected tension pneumothoraces are not infrequently encountered on imaging (Fig. 84.4). Once they are identified, prompt and emergent management is indicated. Fig. 84.1 Fig. 84.2 Radiographically occult pneumothoraces detected on CT in a young man who sustained both head and abdominal trauma following a motor vehicle collision. (A) Supine chest radiography reveals no conspicuous pneumothorax. (B) Abdominal CT (lung window) at the thoraco-abdominal level shows clinically and radiographically unsuspected bilateral pneumothoraces. Fig. 84.3 AP supine chest X-ray of a 16-year-old involved in an ATV rollover shows bilateral ground glass opacities and consolidations, right more so than left, consistent with pulmonary contusions; pneumomediastinum; and subcutaneous air in the chest wall and deep cervical fascia of the neck bilaterally. Persistent left pneumothorax despite chest tube placement is manifest by a crisp left diaphragm and heart border and a deep lateral costophrenic sulcus (deep sulcus sign).
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



