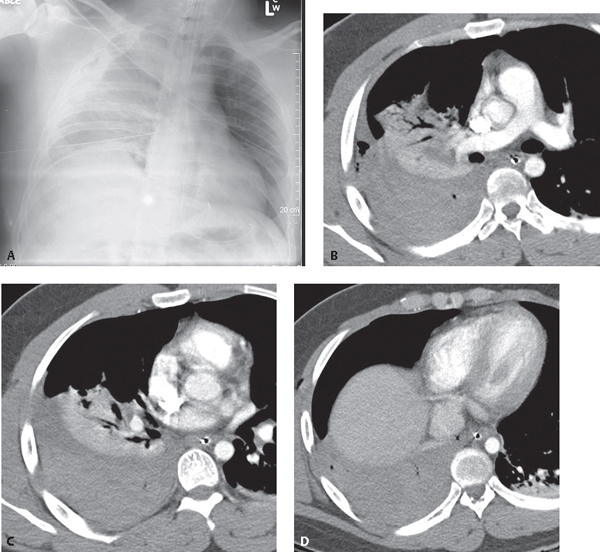
CASE 86 Young male victim of an assault and stabbing to the right chest with diminished breath sounds over the affected thorax. AP chest radiograph (Fig. 86.1A) shows asymmetric hazy ground glass opacification of the right hemithorax from dependent layering pleural fluid. Fluid also tracks along the right lateral chest wall toward the apex. Contrast-enhanced chest CT through the upper (Fig. 86.1B), mid (Fig. 86.1C), and lower (Fig. 86.1D) thorax reveals a large dependent layering, mixed-attenuation pleural fluid collection and relaxation atelectasis in the posterior segment right upper lobe and portions of the middle and lower lobe. Locules of air are present in the pleural space (Figs. 86.1B, 86.1D). Subcutaneous air is seen in the right chest wall (Fig. 86.1D). Fig. 86.1 Hemothorax None Traumatic pleural fluid collections may result from bleeding of the chest wall, mediastinal, or diaphragmatic blood vessels; traumatic central venous catheter line insertions; and thoracic duct injury. Such fluid collections following chest trauma usually represent hemothorax. In fact, hemothorax occurs in approximately 50% of major trauma injuries, especially those caused by penetrating trauma. A small hemothorax also typically occurs in association with post-traumatic ipsilateral pneumothorax. Venous injuries or direct injuries to the lung parenchyma result in low-pressure bleeding with little mass effect and are usually self-limited. Arterial injuries (e.g., intercostals, subclavian, internal mammary) are under greater pressure, may continue to bleed and rapidly fill the affected hemithorax, and may be associated with lung compression and mediastinal displacement. Continued bleeding may require tube thoracostomy drainage.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


