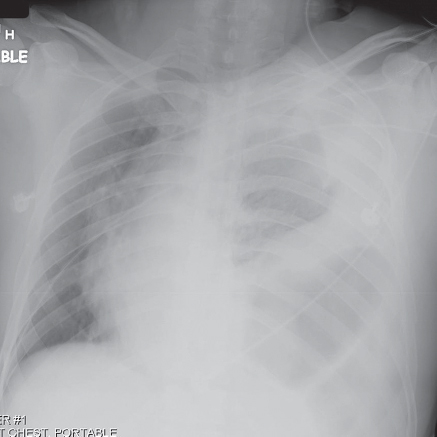
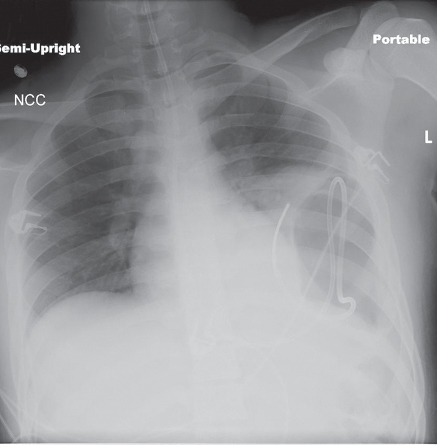
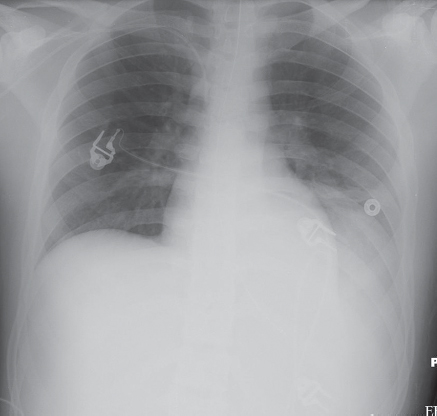
CASE 94 Young man involved in a MVC with respiratory distress and dull breath sounds over the left thorax AP (Fig. 94.1) chest radiograph shows marked rightward displacement of the cardiomediastinal silhouette by herniated hollow viscera into the left thorax. A left-sided hemothorax extends into the apex. Note the large radiolucent focus at the left lung base. Acute Traumatic Rupture Left Diaphragm • Eventration or Elevation of the Diaphragm • Diaphragmatic Paralysis Most diaphragmatic injuries are caused by penetrating trauma. Approximately 15% of stab wounds and 45% of gunshot wounds to the lower chest are complicated by diaphragmatic injuries. Diaphragmatic injuries should be suspected in any penetrating trauma victim with wounds below the fourth anterior, the sixth lateral, and eighth posterior intercostal spaces (4-6-8 rule). The incidence of diaphragmatic injury among blunt trauma victims varies from 0.8% to 8.0% and is more frequently observed with abdominal as opposed to thoracic trauma. Left-sided injuries are three times more common than right-sided injuries; however, as up to 4.5% of blunt trauma victims sustain bilateral diaphragmatic injuries. Most diaphragmatic tears are more than 10 cm in length and involve the muscular posterior or posterolateral diaphragm. Fig. 94.1 A sudden increase in either intra-abdominal or intra-thoracic pressure against a fixed diaphragm accounts for most blunt diaphragmatic injuries. Other postulated mechanisms of injury include shearing stress on a stretched diaphragm and avulsion of the diaphragm from its points of attachment. Acute diaphragmatic injury should be considered in patients who sustain significant abdominal or thoracoabdominal trauma and present with dyspnea or respiratory distress. The majority of affected trauma patients (<94%) have concomitant injuries. Associated injuries often include hepatic (16%) and/or splenic lacerations (48%), rib fractures (52%), pelvic fractures (52%), and closed head injuries (32%). Left-sided diaphragmatic injuries are associated with herniation of subdiaphragmatic viscera into the chest. The stomach and colon are the most commonly herniated organs. As many as three-quarters of affected patients have herniation of other intra-abdominal organs (e.g., omentum, spleen, kidney, pancreas). Diaphragmatic injuries may go unrecognized in patients on positive-pressure ventilation, only declaring their presence following extubation (Fig. 94.2). Delayed herniation may be complicated by bowel strangulation. Intrathoracic splenosis may manifest as a sequela of remote diaphragmatic and splenic injuries on imaging studies decades later and should not be confused with neoplastic disease. Initial chest radiography is diagnostic in 27–60% of left-sided diaphragmatic injuries, but in only 17% of right-sided injuries. • May initially appear normal • Non-specific findings may include: Fig. 94.2 AP chest radiograph of a young trauma victim with delayed presentation of a left diaphragmatic rupture following extubation. Feeding tube is redundantly coiled within the herniated intrathoracic stomach. The patient had been intubated for the past seven days. He was subsequently extubated and the feeding tube was placed in preparation for transfer to a skilled nursing facility because of a concomitant severe closed head injury. Fig. 94.3 AP chest radiograph of a 38-year-old man who sustained a rupture of the left diaphragm following a MVC. Non-specific radiographic signs include a poorly defined, asymmetrically elevated left diaphragm and lower lobe opacification by hemothorax. A 9.0 cm tear was seen intraoperatively and subsequently repaired.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Findings
Chest Radiography
 Elevated asymmetric, poorly visualized, or irregular-appearing diaphragm (Figs. 94.1, 94.2, 94.3)
Elevated asymmetric, poorly visualized, or irregular-appearing diaphragm (Figs. 94.1, 94.2, 94.3)
 Hemothorax, pneumothorax, and hemopneumothorax (Figs. 94.1, 94.2, 94.3)
Hemothorax, pneumothorax, and hemopneumothorax (Figs. 94.1, 94.2, 94.3)
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine




