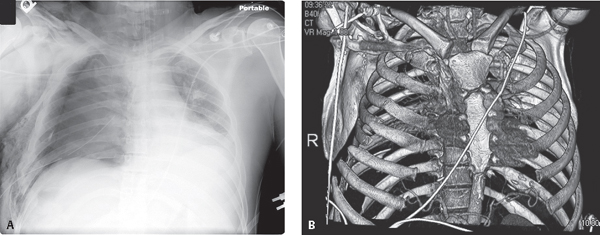
CASE 95 45-year-old pedestrian struck by a bus traveling at approximately 35 mph AP (Fig. 95.1A) chest radiograph reveals a persistent large right pneumothorax despite the chest tube. Diffuse ground glass opacity throughout the right lung consistent with extensive pulmonary contusion. The left lower lobe is collapsed. Multiple contiguous, segmental anterior and posterior right-sided rib fractures are present, many of which are acutely angulated. Extensive subcutaneous air is present in the ipsilateral chest wall. 3-D CT reconstruction (Fig. 95.1B) illustrates the acutely fractured first through eighth anterior and more inferiorly displaced posterior rib fractures to better advantage. Flail Chest with Complicating Bronchial Fracture and Pneumothorax None Rib fractures are the most common injury in blunt chest trauma, occurring in at least 50% of patients. The location and number of involved ribs serve as clues to possible concomitant injuries and to the severity of the trauma. For example, ribs 1–3 are very stable, protected by the shoulder girdle and adjacent musculature. Acute fractures of the upper first three ribs require a substantial force. There is a high correlation of such fractures or fractures of the first two ribs and clavicle with maxillofacial, cranial, brachial plexus, branch vessel, and tracheobronchial injuries. Fractures of ribs 4–9 are common and most significant when associated with flail chest. Fractures of the lower ribs 10–12 are less common but may be associated with traumatic injuries of the liver, spleen, kidneys, and diaphragm. Flail chest is the most severe traumatic injury of the chest wall in blunt trauma. It is characterized by anterior and posterior segmental fractures of more than three congruent ribs or single fractures of more than four contiguous ribs. These fractures create an abnormally mobile, free-floating, unstable chest wall segment that moves paradoxically during the respiratory cycle. The traumatic separation of ribs from their costochondral cartilages (Figs. 95.2A, 95.2B, 95.2C, 95.2D, 95.2E) may also result in a flail segment. Fig. 95.1
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



