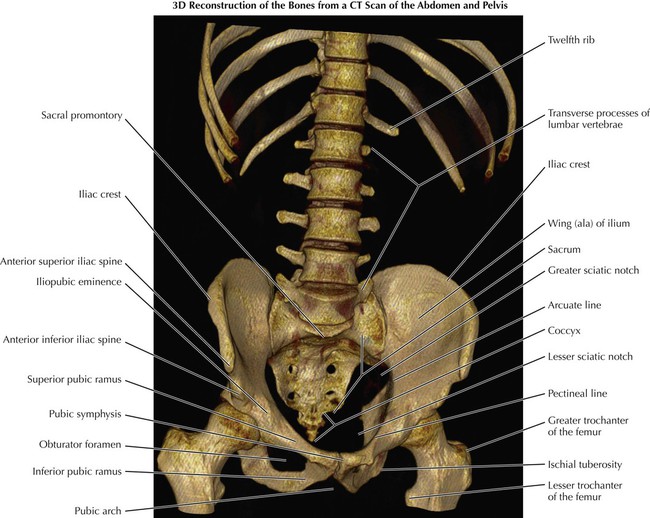
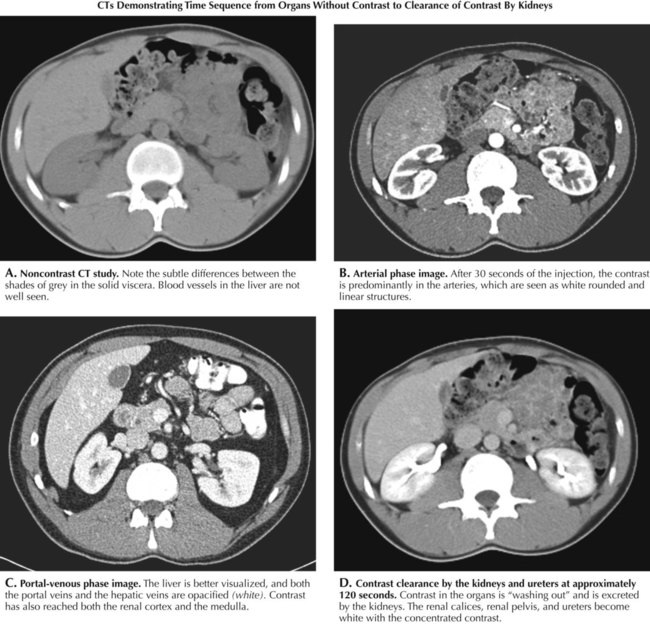
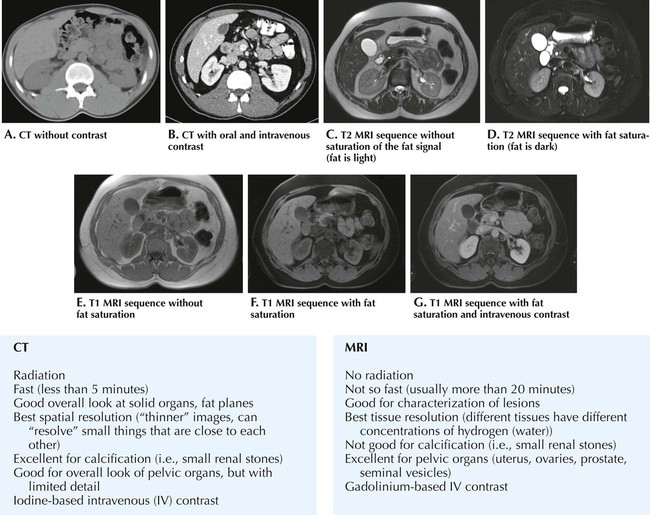
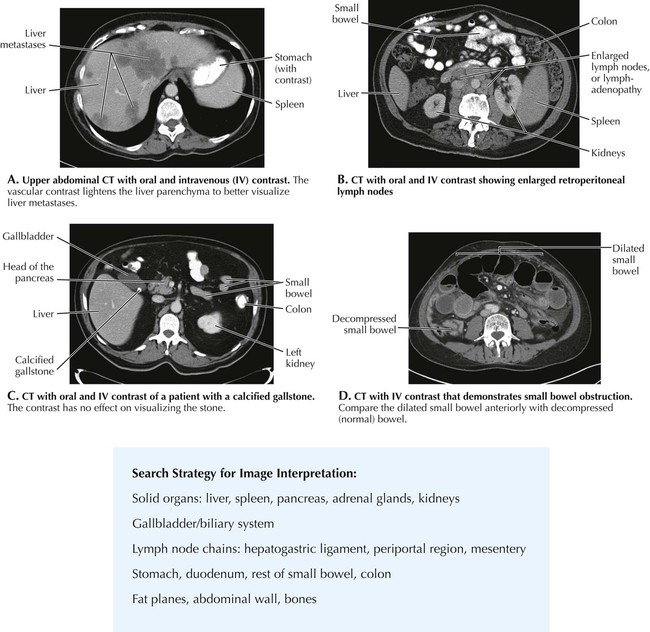
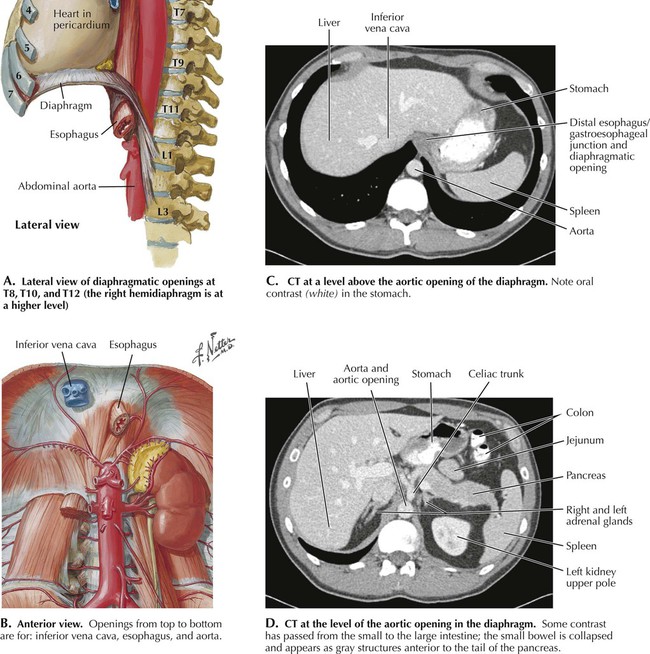
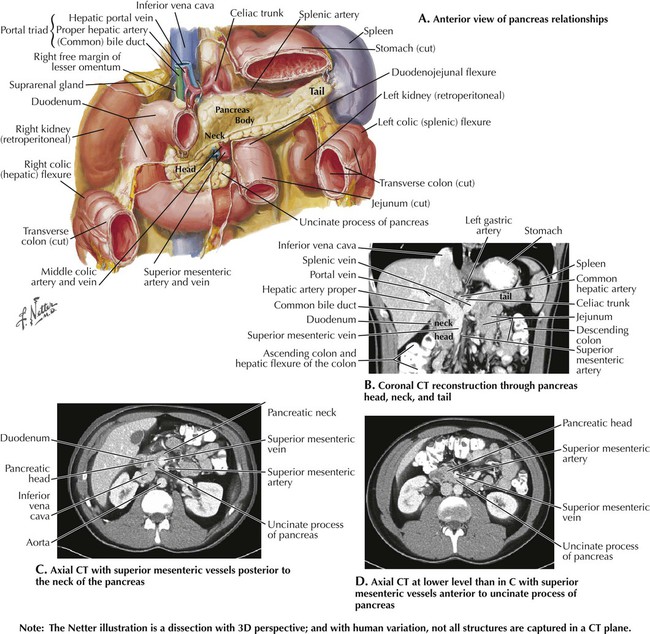
4 Abdomen 4.1. BONY FRAMEWORK: CT THREE-DIMENSIONAL RECONSTRUCTION 4.2. USE OF CONTRAST IN ABDOMINAL IMAGING STUDIES 4.3. CT VS. MRI IN ABDOMINAL STUDIES 4.4. SEARCH STRATEGY: SYSTEMATIC INTERPRETATION OF IMAGING STUDIES 4.5. DIAPHRAGM RELATIONSHIPS 4.6. PANCREAS RELATIONSHIPS 4.7. CROSS SECTION AT T10 WITH CT 4.8. CROSS SECTION AT T12 WITH CT 4.9. CROSS SECTION VARIATION AT T12 WITH CT 4.10. CROSS SECTION AT T12-L1 WITH CT 4.11. CROSS SECTION AT L1-L2 WITH CT 4.12. KIDNEY RELATIONSHIPS 4.13. L3-L4 CROSS SECTION WITH CT 4.14. SAGITTAL SECTION THROUGH AORTA WITH CT SAGITTAL RECONSTRUCTION 4.15. STOMACH IN SITU 4.16. UPPER GASTROINTESTINAL CT STUDIES 4.17. HIATAL HERNIA 4.18. LARGE INTESTINE IMAGING STUDIES 4.19. GALLBLADDER, BILE DUCTS, AND PANCREATIC DUCT 4.20. ABDOMINAL FOREGUT ARTERIES 4.21. MIDGUT AND HINDGUT ARTERIES 4.22. ANGIOGRAMS OF THE SUPERIOR AND INFERIOR MESENTERIC VESSELS 4.23. PERITONEAL/RETROPERITONEAL RELATIONSHIPS 4.24. GASTROINTESTINAL PATHOLOGY 4.1 Bony Framework: CT Three-Dimensional Reconstruction This three-dimensional (3D) image is reconstructed with a computer from individual computed tomography (CT) axial images, much like a pile of flat rings form a cylinder. Radiologists may not use images like this routinely for diagnosis, but it is very helpful for surgeons to have a 3D plan of the anatomy to reconstruct fractured bones. Cartilage is not demonstrated on the image because it is not as radiopaque as bone. Without the mineral content of bone, cartilage has a density similar to that of water and soft tissues. 4.2 Use of Contrast in Abdominal Imaging Studies Computed tomography can be performed with or without oral and/or intravenous (IV) contrast. Oral contrast helps the evaluation of the hollow viscera; agents include water, barium, and iodinated contrast. IV contrast is used to better evaluate the solid viscera, lesions, vasculature, and wall of the hollow viscera. Iodinated contrast is injected into a vein, usually an antecubital vein. It goes to the heart, to the lungs, and then to the aorta, which appears white from the contrast. In B, note that contrast has also reached arteries in the renal cortex, which is also white. As time goes by, the contrast is drained by veins in the organs, and everything becomes a little lighter shade of gray (C) compared to a noncontrast study. The contrast is filtered by the kidneys and opacifies the renal collecting systems, which become very bright (white) from the concentrated contrast (D). 4.3 CT vs. MRI in Abdominal Studies These figures give an overview of the differences in appearance in a variety of CT and magnetic resonance imaging (MRI) sequences. A T2-weighted sequence is very fluid sensitive, and the fluid is seen as white. In T1-weighted sequences the fluid is dark. Settings for fat saturation (where fat is dark) help to identify edema (swelling from fluid accumulation) and hemorrhage and distinguish them from fat. Fat saturation also helps to identify lesions that are located within the fat and bone marrow, plus other pathology. Usually several sequences are needed to obtain a diagnosis. 4.4 Search Strategy: Systematic Interpretation of Imaging Studies As with each body region, every radiologist has his or her own search pattern to interpret a study. The table in this figure contains a useful sequence to follow to look for pathology in a systematic way. Each organ is inspected in great detail before going to the next. Examples of pathology are given in the four figures. 4.5 Diaphragm Relationships These figures emphasize the relationships between abdominal organs and the position of the diaphragm. The abdominal cavity extends under the diaphragm to the T8 vertebral level, where the inferior vena cava passes through the central tendon of the right hemidiaphragm. The esophagus passes through its muscle at T10, and the aorta through the crura at T12, where the celiac trunk branches originate. In (C), the liver, stomach and spleen are prominent in the image; but the origin of their arteries off the celiac trunk is at a lower level (D). The T8, T10, and T12 openings for the three large structures are averages. There is considerable individual variation plus variation caused by posture and position of the diaphragm in the breathing cycle. 4.6 Pancreas Relationships The pancreas has anatomical relationships that are clinically important and useful in the identification of structures in the abdominal foregut. The head of the pancreas lies in the curve of the duodenum, and its tail courses upward to the spleen. The celiac trunk originates just above the pancreas, and the splenic artery and vein follow the body and tail of the pancreas to the spleen, giving off numerous pancreatic branches along the way. The superior mesenteric artery originates immediately below the celiac trunk posterior to the neck of the pancreas. It appears medial to the head of the pancreas and passes anterior to the uncinate (“hooklike”) process, the most inferior extent of the pancreas. The portal vein is formed behind the pancreas by the union of the splenic and superior mesenteric veins. The common bile duct joins the pancreatic duct in the head of the pancreas to form the ampulla in the second part of the duodenum. 4.7 Cross Section at T10 with CT The CT image is at the level of the inferior endplate of T11, but it corresponds closely to the T10 Netter illustration (A). Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Introduction to Imaging Modalities Back and Spinal Cord Upper Limbs Lower Limbs Thorax Head and Neck Stay updated, free articles. Join our Telegram channel Join Tags: Netters Introduction to Imaging Jan 10, 2016 | Posted by admin in RADIOGRAPHIC ANATOMY | Comments Off on Abdomen Full access? Get Clinical Tree
4 Abdomen 4.1. BONY FRAMEWORK: CT THREE-DIMENSIONAL RECONSTRUCTION 4.2. USE OF CONTRAST IN ABDOMINAL IMAGING STUDIES 4.3. CT VS. MRI IN ABDOMINAL STUDIES 4.4. SEARCH STRATEGY: SYSTEMATIC INTERPRETATION OF IMAGING STUDIES 4.5. DIAPHRAGM RELATIONSHIPS 4.6. PANCREAS RELATIONSHIPS 4.7. CROSS SECTION AT T10 WITH CT 4.8. CROSS SECTION AT T12 WITH CT 4.9. CROSS SECTION VARIATION AT T12 WITH CT 4.10. CROSS SECTION AT T12-L1 WITH CT 4.11. CROSS SECTION AT L1-L2 WITH CT 4.12. KIDNEY RELATIONSHIPS 4.13. L3-L4 CROSS SECTION WITH CT 4.14. SAGITTAL SECTION THROUGH AORTA WITH CT SAGITTAL RECONSTRUCTION 4.15. STOMACH IN SITU 4.16. UPPER GASTROINTESTINAL CT STUDIES 4.17. HIATAL HERNIA 4.18. LARGE INTESTINE IMAGING STUDIES 4.19. GALLBLADDER, BILE DUCTS, AND PANCREATIC DUCT 4.20. ABDOMINAL FOREGUT ARTERIES 4.21. MIDGUT AND HINDGUT ARTERIES 4.22. ANGIOGRAMS OF THE SUPERIOR AND INFERIOR MESENTERIC VESSELS 4.23. PERITONEAL/RETROPERITONEAL RELATIONSHIPS 4.24. GASTROINTESTINAL PATHOLOGY 4.1 Bony Framework: CT Three-Dimensional Reconstruction This three-dimensional (3D) image is reconstructed with a computer from individual computed tomography (CT) axial images, much like a pile of flat rings form a cylinder. Radiologists may not use images like this routinely for diagnosis, but it is very helpful for surgeons to have a 3D plan of the anatomy to reconstruct fractured bones. Cartilage is not demonstrated on the image because it is not as radiopaque as bone. Without the mineral content of bone, cartilage has a density similar to that of water and soft tissues. 4.2 Use of Contrast in Abdominal Imaging Studies Computed tomography can be performed with or without oral and/or intravenous (IV) contrast. Oral contrast helps the evaluation of the hollow viscera; agents include water, barium, and iodinated contrast. IV contrast is used to better evaluate the solid viscera, lesions, vasculature, and wall of the hollow viscera. Iodinated contrast is injected into a vein, usually an antecubital vein. It goes to the heart, to the lungs, and then to the aorta, which appears white from the contrast. In B, note that contrast has also reached arteries in the renal cortex, which is also white. As time goes by, the contrast is drained by veins in the organs, and everything becomes a little lighter shade of gray (C) compared to a noncontrast study. The contrast is filtered by the kidneys and opacifies the renal collecting systems, which become very bright (white) from the concentrated contrast (D). 4.3 CT vs. MRI in Abdominal Studies These figures give an overview of the differences in appearance in a variety of CT and magnetic resonance imaging (MRI) sequences. A T2-weighted sequence is very fluid sensitive, and the fluid is seen as white. In T1-weighted sequences the fluid is dark. Settings for fat saturation (where fat is dark) help to identify edema (swelling from fluid accumulation) and hemorrhage and distinguish them from fat. Fat saturation also helps to identify lesions that are located within the fat and bone marrow, plus other pathology. Usually several sequences are needed to obtain a diagnosis. 4.4 Search Strategy: Systematic Interpretation of Imaging Studies As with each body region, every radiologist has his or her own search pattern to interpret a study. The table in this figure contains a useful sequence to follow to look for pathology in a systematic way. Each organ is inspected in great detail before going to the next. Examples of pathology are given in the four figures. 4.5 Diaphragm Relationships These figures emphasize the relationships between abdominal organs and the position of the diaphragm. The abdominal cavity extends under the diaphragm to the T8 vertebral level, where the inferior vena cava passes through the central tendon of the right hemidiaphragm. The esophagus passes through its muscle at T10, and the aorta through the crura at T12, where the celiac trunk branches originate. In (C), the liver, stomach and spleen are prominent in the image; but the origin of their arteries off the celiac trunk is at a lower level (D). The T8, T10, and T12 openings for the three large structures are averages. There is considerable individual variation plus variation caused by posture and position of the diaphragm in the breathing cycle. 4.6 Pancreas Relationships The pancreas has anatomical relationships that are clinically important and useful in the identification of structures in the abdominal foregut. The head of the pancreas lies in the curve of the duodenum, and its tail courses upward to the spleen. The celiac trunk originates just above the pancreas, and the splenic artery and vein follow the body and tail of the pancreas to the spleen, giving off numerous pancreatic branches along the way. The superior mesenteric artery originates immediately below the celiac trunk posterior to the neck of the pancreas. It appears medial to the head of the pancreas and passes anterior to the uncinate (“hooklike”) process, the most inferior extent of the pancreas. The portal vein is formed behind the pancreas by the union of the splenic and superior mesenteric veins. The common bile duct joins the pancreatic duct in the head of the pancreas to form the ampulla in the second part of the duodenum. 4.7 Cross Section at T10 with CT The CT image is at the level of the inferior endplate of T11, but it corresponds closely to the T10 Netter illustration (A). Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Introduction to Imaging Modalities Back and Spinal Cord Upper Limbs Lower Limbs Thorax Head and Neck Stay updated, free articles. Join our Telegram channel Join Tags: Netters Introduction to Imaging Jan 10, 2016 | Posted by admin in RADIOGRAPHIC ANATOMY | Comments Off on Abdomen Full access? Get Clinical Tree