pelvis.1 Passengers in a vehicle struck on the right side are prone to right-sided injuries, including right rib fractures, right lung contusions and lacerations, lacerations of the right lobe of the liver and right kidney, and pelvic fractures. Passengers are less prone to thoracic injuries and more prone to abdominal injuries than are drivers.1
Life-threatening, trauma-specific
Hemoperitoneum
Pneumothorax (lung windows)
Pneumoperitoneum (lung windows)
Hemodynamic status
Active arterial contrast extravasation
Liver and right paracolic gutter
Spleen and left paracolic gutter
Upper abdominal organs, including duodenum and pancreas
Retroperitoneum, including adrenals, kidneys, inferior vena cava, and aorta
Bowel and mesentery
Pelvis
Muscles, including abdominal wall, psoas, iliacus, and buttocks
Bones (bone windows)
Lowest cut (thigh hematoma)
 Figure 15.1. Grade II splenic laceration with sentinel clot. A: At the upper pole of the spleen, the lateral surface is lacerated (solid arrow). A high-attenuation blood clot (C) floats in the nondependent portion of the perisplenic space—the sentinel clot sign. Low-attenuation fluid is present in the right perihepatic space (open arrows). The electrocardiographic electrode over the left anterior chest causes a moderate streak artifact. B: In the hepatorenal recess, hemoperitoneum (open arrows) is only slightly higher in attenuation than the renal cyst lateral to the left kidney (curved arrow). Intraperitoneal fluid in the hepatorenal recess typically wraps around the tip of the liver, distinguishing it from retroperitoneal fluid. |
capabilities available with MDCT and is more prone to respiratory motion artifacts. Administration of intravenous contrast medium is mandatory to detect all possible injuries. Unenhanced CT is performed rarely in trauma, limited to patients with a well-documented severe allergy to contrast material. Evaluation of vessels and solid organs is not complete unless intravenous contrast material is administered. Patient preparation is very important but must be accomplished efficiently. To minimize streak artifacts, metal objects within the scanning field should be removed or repositioned, including metal buckles on patient restraints, belts, electrocardiography electrodes (Fig. 15.1) and connecting cables, and metal or metal-reinforced backboards (Fig. 15.2). Some backboards cause such severe artifacts that the patient should be transferred to a more “CT friendly” wooden or plastic backboard. Once the patient is on the CT table, the patient’s upper extremities should be raised above the head to avoid streak artifact. When upper extremity injuries preclude repositioning of the arms, placing the upper extremity close to the patient’s side and enlarging the scanning field to include the upper extremity reduces artifacts. Alert and cooperative patients should hold their breath during the imaging of the upper abdomen to minimize respiratory motion artifacts. However, successful breath holding is often not possible and scanning during shallow, quiet breathing is often necessary.
TABLE 15.1 Grading Criteria for Abdominal and Retroperitoneal Injury | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
 Figure 15.2. Streak artifact from backboard. At the splenic hilum and tip of the liver, severe streak artifact is so severe that the hemoperitoneum around the spleen is difficult to diagnose (straight arrows). The patient’s upper extremities at his side, the metal struts of the backboard, and respiratory motion cause the image degradation. Note the bright halo around the lateral portion of the right kidney, which simulates a subcapsular hematoma (curved arrow). |
1 to 1.25 mm and 3.75 to 5 mm section thicknesses are provided for interpretation. Orthogonal (coronal and sagittal) reformations are generated for all patients for all series acquired, both with 2.5-mm thickness and 2.5-mm reconstruction interval.
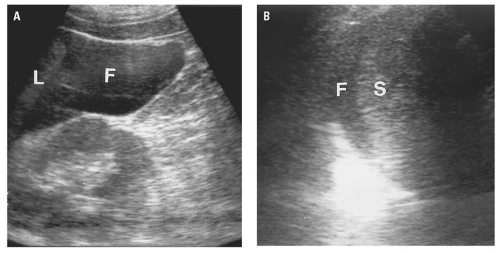 Figure 15.3. Hemoperitoneum. A: Longitudinal ultrasound image of the right upper quadrant obtained with a 3.5 MHz curved-array transducer demonstrates fluid (F) with low-level internal echoes in the hepatorenal recess adjacent to the tip of the liver (L). B: In a different patient, echogenic fluid (F) is present between the diaphragm and the upper pole of the spleen (S). |
 Figure 15.4. Pneumoperitoneum. In the midabdomen, a collection of free intraperitoneal air separates the parietal peritoneum of the anterior abdominal wall from the visceral peritoneum of the greater omentum (straight arrows). Air within an adjacent jejunal loop (curved arrow) surrounds thickened valvulae conniventes, which clearly establishes its intraluminal location. |
Bubbles of free air may be trapped between leaves of mesentery or in the peritoneal recesses. Lung windows are valuable in detecting pneumoperitoneum, which might be overlooked on soft tissue windows because free air may not be distinguishable from adjacent bowel gas at narrow window widths.
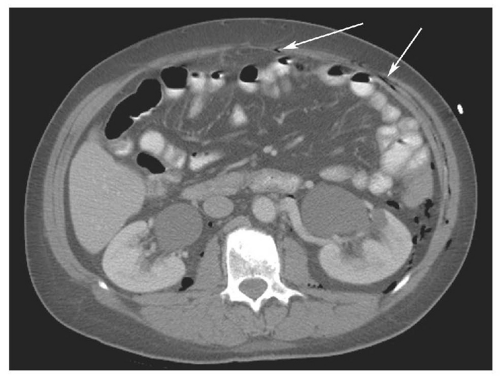 Figure 15.5. 58-year-old female patient with a pelvic fracture and a rectal wall tear, allowing leakage of gas into the extraperitoneal space of the pelvis. The axial CT image demonstrates gas in the retroperitoneum (surrounding the kidneys and descending colon) as well as in the extraperitoneal space of the anterior abdominal wall (“pseudopneumoperitoneum,” arrows). The patient underwent repair of the rectal tear, but no laparotomy was performed. |
hemoperitoneum may be estimated by searching for fluid in the perisplenic space, perihepatic space, hepatorenal recess, right and left paracolic gutters, and pelvis.46 Small collections of fluid are confined to one space; moderate collections are seen in two or more spaces; and large collections involve all spaces. Although the volume of hemoperitoneum will have an effect on patient management decisions, a large hemoperitoneum does not mandate laparotomy.10, 17
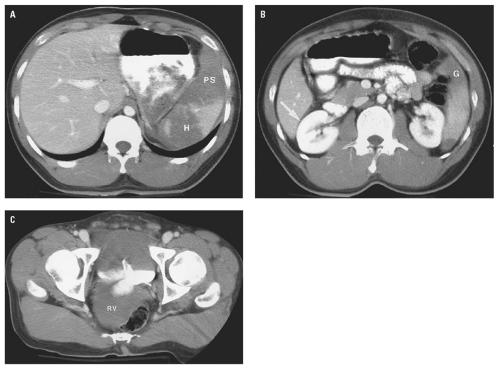 Figure 15.6. Grade IV splenic laceration with left-sided hemoperitoneum. A: Above the splenic hilum, the spleen is fragmented. Intraparenchymal hematoma (H) separates the fragments. Hemoperitoneum distends the perisplenic space (PS). B: At the lower pole, the hemoperitoneum enters the upper portion of the left paracolic gutter (G), but no hemoperitoneum is present in the hepatorenal recess (arrow). C: In the pelvis, hemoperitoneum fills the rectovesical space (RV). |
for detecting small amounts of free intraperitoneal fluid has improved, and the radiologist must use all the tools available to help guide further management.
 Figure 15.7. Isolated low attenuation free fluid. Coronal CT reformation demonstrates a small amount of low attenuation fluid (measured at 8 HU) in the pelvis (arrow). No additional findings to indicate presence of a solid organ or hollow viscus injury were present. The patient was treated conservatively and had an uneventful hospital stay. |
anomalies, or portosystemic shunting. Flattening of the IVC is encountered in outpatients undergoing CT for nontrauma reasons.60 However, in a hemorrhaging trauma patient, a flattened IVC indicates inadequate volume resuscitation. IVC flattening may precede clinical signs of shock. Recognition of intravascular volume depletion on CT should prompt aggressive volume resuscitation before the patient develops more overt signs of cardiovascular collapse.
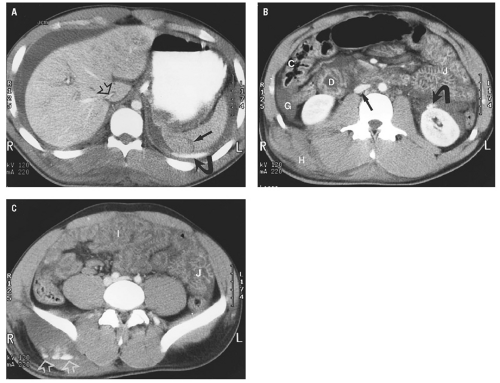 Figure 15.8. Splenic laceration with the hypoperfusion complex and active arterial extravasation in an 18-month-old infant. A: Image through the spleen demonstrates a grade II splenic laceration (straight arrow) with adjacent active arterial extravasation (curved arrow) and abundant hemoperitoneum surrounding the liver and spleen. Note the slit-like IVC (open arrow) as it passes through the liver. B: In the midabdomen, the duodenum (D), jejunum (J), and ascending colon (C) all have thickened walls and abnormally enhancing mucosa. Hemoperitoneum is seen in the right paracolic gutter (G). Active arterial extravasation from the anterior surface of the left kidney (curved arrow) results in a perinephric hematoma. The IVC (straight arrow) is flattened and the adjacent aorta is relatively small. A large hematoma (H) is present in the right flank. C: In the upper pelvis, abnormal mucosal enhancement is noted in the jejunum (J) and, to a lesser degree, the ileum (I). Active arterial extravasation is seen in the right buttocks (open arrows). (Case courtesy of Steven Ashlock, MD) |
posterior segment of the right lobe most frequently injured.62 Most liver injuries cause hemoperitoneum, but approximately one-fifth do not.63 Liver injuries that do not produce hemoperitoneum will usually be missed by FAST, except in the unusual circumstance that a parenchymal laceration is seen directly by ultrasound. Liver injuries presenting without hemoperitoneum include minor liver injuries that do not cause significant bleeding, injuries that cause purely intraparenchymal hematoma, and injuries that disrupt the surface of the bare area of the liver and cause retroperitoneal hemorrhage.64
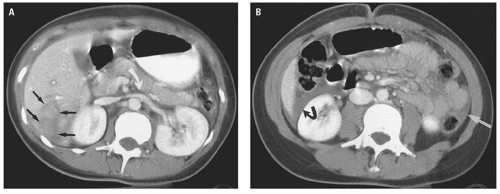 Figure 15.9. Grade III laceration of segments V and VI and complete pancreatic body laceration. A: Image through the right lobe of the liver shows a deep laceration extending to a portal vein branch in segment VI (straight black arrows). A hairline fracture is seen through the entire thickness of the pancreatic body (straight white arrows). Fluid between the pancreas and splenic vein (curved white arrow) indicates that this is a true pancreatic injury rather than a streak artifact over the pancreas. B: At the hepatorenal recess, hemoperitoneum (curved black arrow) surrounds the tip of the liver. Note a small amount of blood in the left paracolic gutter (white arrow). |
to be associated with biliary tract injuries.66 Lacerations extending to the proximal hepatic veins are important to identify because repair of hepatic vein injuries is technically difficult.67
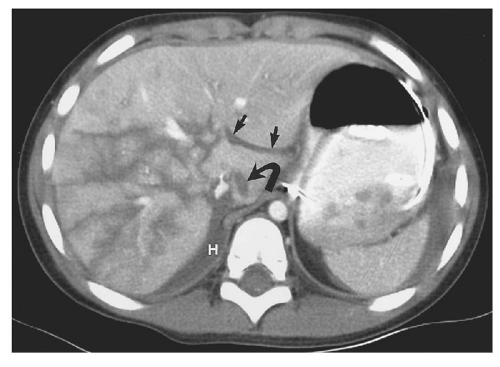 Figure 15.10. Grade V laceration of the entire right lobe of the liver. Multiple lacerations in a stellate pattern involve the entire right lobe of the liver, including the proximal portal vein branches and the intrahepatic IVC. Note retroperitoneal hematoma between the liver and the right hemidiaphragm (H) caused by lacerations involving the bare area. The fissure for the ligamentum venosum is filled with blood (straight arrows). Laceration in the caudate lobe is an unusual finding (curved arrow). |
 Figure 15.11. “Bear claw” liver laceration. Complex lacerations involving the left and right hepatic lobes, and extending to the porta hepatis. |
 Figure 15.12. Grade II liver laceration (arrow) without associated hemoperitoneum. |
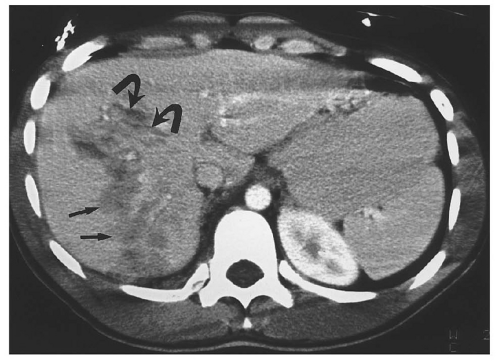 Figure 15.13. Hepatic contusion. The poorly defined area of low attenuation in the right lobe represents hepatic contusion (straight arrows). More well-defined lacerations are seen anteriorly (curved arrows). |
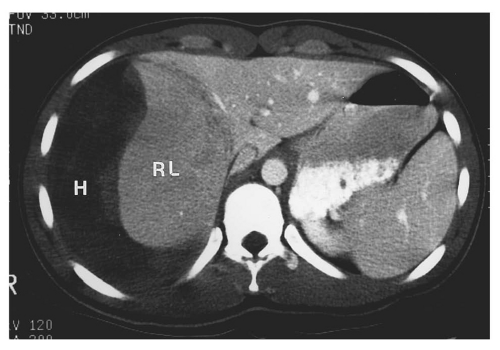 Figure 15.14. Large subcapsular hematoma of the liver. Above the porta hepatis, a large subcapsular hematoma (H) deforms the right lobe of the liver (RL). Note that the right lobe has diminished parenchymal enhancement compared to the left, probably due to the pressure exerted by the hematoma. (Case courtesy of Steven Ashlock, MD) |
 Figure 15.15. Grade III-IV laceration of the right lobe with active arterial extravasation. Above the porta hepatis, a deep laceration involving segment VII has a focus of active hemorrhage at its base (curved arrow). Note the jet of active arterial extravasation extending to the periphery (straight arrows). Relatively dense blood is seen adjacent to the liver—the sentinel clot sign (C). |
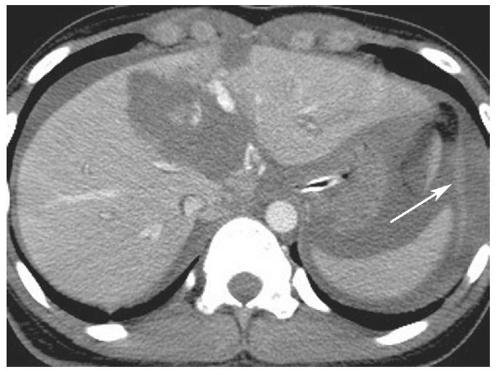 Figure 15.16. Massive liver laceration involving the right and left lobes, with large foci of intraparenchymal active extravasation as well as extravasation into the perisplenic space (arrow). Note also abundant hemoperitoneum. |
 Figure 15.17. Unopacified middle hepatic vein simulating a liver laceration. This image was made in the early vascular phase before there was filling of the portal or hepatic veins. The middle hepatic vein (arrows) could be mistaken for a deep laceration. |
TABLE 15.2 American Association for the Surgery of Trauma Liver Injury Scale (1994 revision) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||