Usually result from injection of subcutaneous heparin, self-injection of insulin, etc.
Low-density nodules associated with ectopic gas or fluid
• Injection or incision site hematoma or seroma
May be misinterpreted as neoplasm but should resolve over time
• Injection or incision site abscess
Suspicious imaging features include peripheral enhancement, surrounding soft tissue edema and stranding (i.e., cellulitis), and internal ectopic gas
• Diabetic lipodystrophy
Insulin-dependent diabetic patients may develop atrophy or hypertrophy of fat at injection sites
Lipohypertrophy appears as mixed fatty mass in subcutaneous tissue on CT or MR
• Keloid (hypertrophic scar)
Benign fibrotic scar tissue or soft tissue overgrowth at site of healed skin injury (i.e., incisional scar)
No clear distinguishing imaging features
• Calcified or ossified scar
Abdominal incision may develop cartilaginous, osseous, or myelogenous (bone marrow) elements
• Endometrial implantation in abdominal incision
Most often seen after cesarean section (80% of cases)
Cyclical pain at incision site with menstruation
Lesions appear solid and irregularly shaped/spiculated on CT or MR with moderate enhancement
• Tumor implantation in incision sites
Probably more common after laparoscopic surgery
Nonspecific imaging appearance, with soft tissue density mass near or within incision site
• Injection granulomas
Sequelae of subcutaneous injection of drugs resulting in local fat necrosis, scarring, and calcification
Usually rounded or linear soft tissue or calcific density lesion seen in subcutaneous fat of buttocks
(Left) Plain film radiograph shows rounded calcifications that overlap the lower abdomen. Some of these are lateral to the descending colon and close to the skin, establishing their extraabdominal location.
(Right) Axial NECT in the same patient shows heavily calcified injection sites in the subcutaneous tissues over the buttocks. Renal failure may have contributed to the deposition of so much calcium in these lesions.
(Left) Axial CECT shows a heavily calcified or ossified upper abdominal incision site immediately caudal to the xiphoid process.
(Right) Coronal CECT in another patient shows a long ossification (over 10 cm) of the midline incision site . The appearance is very similar to that of a rib, with both the cortex and medulla clearly seen.
TERMINOLOGY
Definitions
• Lesions in abdominal wall at either incision or injection sites that may be mistaken for other pathologic conditions
IMAGING
General Features
• Best diagnostic clue
• Size
• Morphology
Imaging Recommendations
• Best imaging tool
CT
Radiographic Findings
Injection Site Fluid or Gas Collection
• Very common finding in subcutaneous tissues of anterior abdominal wall
Usually associated with injection of subcutaneous heparin, self-injection of insulin, etc.
• Usually appear as small, low-density nodular foci associated with small ectopic gas, fluid, or blood products
• May be misinterpreted as hematoma, abscess, or soft tissue infection but usually has little fluid and resolves quickly
Injection or Incision Site H
• Hematoma: Heterogeneous, high-attenuation (> 60 HU) mass in abdominal wall
• Seroma: Lower density, more homogeneous collection of fluid without peripheral enhancement
• May be misinterpreted as neoplasm (i.e., tumor implant at incision or laparoscopic port following surgical resection of malignancy), but imaging appearance is usually characteristic and should resolve over time
Injection or Incision Site A
• May be indistinguishable from uninfected hematoma or seroma
May require needle aspiration and fluid analysis in cases with high clinical suspicion
• Suspicious imaging features for abscess include peripheral enhancement, worsening surrounding soft tissue edema and stranding (i.e., cellulitis), and internal foci of ectopic gas
Diabetic Lipodystrophy
• Insulin-dependent diabetic patients may develop atrophy or hypertrophy of fat at insulin injection sites
Can be seen less commonly with several other drugs, including injected steroids (atrophy), octreotide (atrophy), and IGF-1 (hypertrophy)
• Injection site lipoatrophy
Loss of fat at sites of repeated insulin injections
May be caused by allergic response to insulin, but now less common with use of human insulin
• Injection site lipohypertrophy
Proliferation of fat and fibrous tissue at site of repeated injections
– Common problem that is estimated to occur in almost 50% of insulin-dependent patients to some extent
– Easier to palpate than to see visually or by imaging
Forms palpable lump in subcutaneous tissues resembling miniature breast
– Caused by repeated injections at 1 site without rotation to others
Patients may prefer to do so as injections into sites of lipohypertrophy are less painful
Absorption of insulin at these sites is erratic
Nurses caring for diabetic patients are very familiar with this and should encourage patients to change injection sites frequently to avoid this problem
Only gold members can continue reading. Log In or Register to continue





 Benign fibrotic scar tissue or soft tissue overgrowth at site of healed skin injury (i.e., incisional scar)
Benign fibrotic scar tissue or soft tissue overgrowth at site of healed skin injury (i.e., incisional scar)






 Sequelae of subcutaneous injection of drugs resulting in local fat necrosis, scarring, and calcification
Sequelae of subcutaneous injection of drugs resulting in local fat necrosis, scarring, and calcification

 that overlap the lower abdomen. Some of these are lateral to the descending colon and close to the skin, establishing their extraabdominal location.
that overlap the lower abdomen. Some of these are lateral to the descending colon and close to the skin, establishing their extraabdominal location.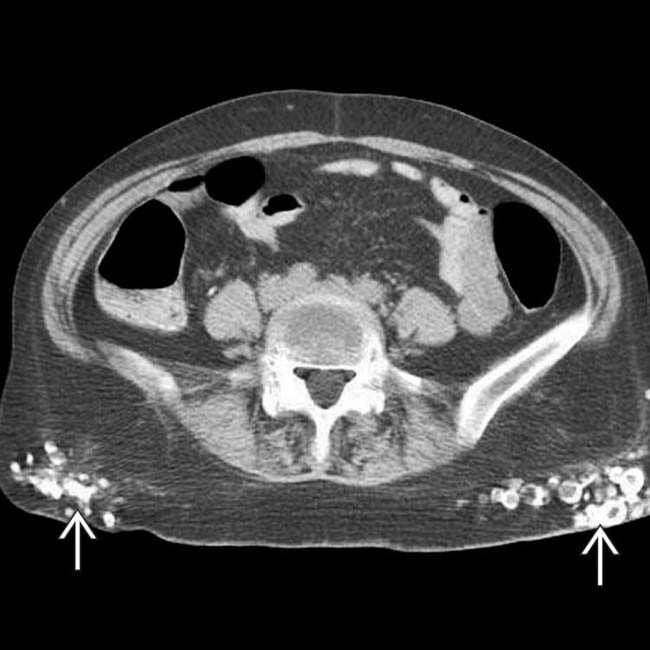
 in the subcutaneous tissues over the buttocks. Renal failure may have contributed to the deposition of so much calcium in these lesions.
in the subcutaneous tissues over the buttocks. Renal failure may have contributed to the deposition of so much calcium in these lesions.
 immediately caudal to the xiphoid process.
immediately caudal to the xiphoid process.
 . The appearance is very similar to that of a rib, with both the cortex and medulla clearly seen.
. The appearance is very similar to that of a rib, with both the cortex and medulla clearly seen.








 Proliferation of fat and fibrous tissue at site of repeated injections
Proliferation of fat and fibrous tissue at site of repeated injections
 Nurses caring for diabetic patients are very familiar with this and should encourage patients to change injection sites frequently to avoid this problem
Nurses caring for diabetic patients are very familiar with this and should encourage patients to change injection sites frequently to avoid this problem







