Case presentation
A previously healthy 14-year-old male presents with left lower quadrant pain, difficulty bearing weight, and fever. He awoke 6 days ago with sharp left lower quadrant pain. At that time, he was seen at an Emergency Department where abdominal computed tomography (CT) and bloodwork were obtained, which were reported to be normal. He was diagnosed with abdominal wall strain and was discharged home with ibuprofen. He reports that this medication has not helped his pain. He went to his primary care provider the following day, who diagnosed mesenteric adenitis and prescribed hydrocodone. The patient reports that the pain has persisted despite this additional medicine. Several days ago, he developed fever, which has been intermittent since then. He states that he has had progressive difficulty with ambulation secondary to pain. He returned to his primary care provider 2 days ago, who obtained plain radiography of the pelvis, which was normal by report. He has not had preceding trauma, although he states that he is a track and field runner, has an extensive exercise routine, and is unsure if he “pulled something” prior to his current symptoms. He denies vomiting, diarrhea, dysuria, or back pain.
He is febrile to 103 degrees Fahrenheit, has a pulse of 106 beats per minute, a respiratory rate of 24 breaths per minute, and a blood pressure of 109/54 mm Hg. He is not in distress but complains of left-sided hip pain, radiating to the left anterior thigh. His abdominal examination reveals tenderness to the left lower quadrant without rebound or guarding. He has exquisite pain with manipulation of his left leg, pointing to the left hip and left thigh. There is no erythema, swelling, fluctuance, or warmth, but he is tender to palpation over the left anterior thigh.
A review of the outside CT report does not mention any abnormalities. Laboratory work is obtained, revealing a total white blood cell count of 15,000 cc/mm, normal urinalysis, a C-reactive protein (CRP) level of 35 mg/dL, an erythrocyte sedimentation rate (ESR) of 90 mm/hour, and a creatine phosphokinase (CK) level of 299 units/L.
Imaging considerations
Plain radiography
This imaging modality is the first-line choice for patients presenting with musculoskeletal complaints. Plain radiography is useful in detecting fractures, radio-opaque foreign bodies, tumors, and changes associated with infection, such as osteomyelitis. It is readily available, exposes the patient to minimal amounts of ionizing radiation, and does not require sedation to complete a meaningful study.
Computed tomography
This modality can identify fluid collections and the contents of the collection and assist in determining if an abscess exists. Pyomyositis on CT imaging may demonstrate enlargement and decreased attenuation of the affected muscle with effacement of surrounding fat planes. The presence of disproportionate muscular involvement compared to subcutaneous soft tissue can help to distinguish pyomyositis from cellulitis. Using intravenous contrast material, a rim-enhancing abscess may be identified. This modality may be useful to help guide drainage of an identified abscess.
However, CT is inferior to magnetic resonance imaging (MRI) for soft tissue infection evaluation and is not the recommended follow-up study in these patients. If soft tissue or bone infection is suspected, then MRI is the modality of choice.
Magnetic resonance imaging
MRI has excellent capability in identifying fluid collections such as an abscess and associated anatomy surrounding the abscess. , , This modality, preferably with imaging with and without intravenous contrast, is the imaging study of choice for patients with suspected soft tissue infections, including pyomyositis, and bone infections. T1-weighted images demonstrate localized areas of hypointensity and T2-weighted images demonstrate hyperintense areas; with abscess, gadolinium-enhanced images will demonstrate an enhancing peripheral rim surrounding a fluid collection, without central enhancement of fluid contents. Limitations for use of MRI include availability and the likely need for sedation in younger patients.
Ultrasound (US)
There are several advantages to this imaging modality: availability, lack of ionizing radiation, no requirement for intravenous contrast, and US can identify soft tissue foreign bodies. US has proven useful in assisting with the diagnosis of soft tissue infections; in one study, it outperformed physical examination in the detection of patients with this diagnosis. , There are reports on the use of US to successfully diagnose pyomyositis in adult patients. , On US, an abscess may show localized edema, linear plane distortion, and a hypoechoic center area, but this center may be more complex in echotexture. Compression of the abscess during imaging may allow confirmation of fluid contents and may show mobile purulent material. , , There are limitations to the use of US in patients with suspected soft tissue infection. This modality is operator dependent. Due to the depth of the abscess in pyomyositis (involving the muscle layer), the clinician employing US should identify the striation of muscle to ensure proper visualization of the muscle layers. US may also underestimate the size of the abscess, and while US can detect fluid collections, identifying the contents of the collection can be difficult.
Imaging findings
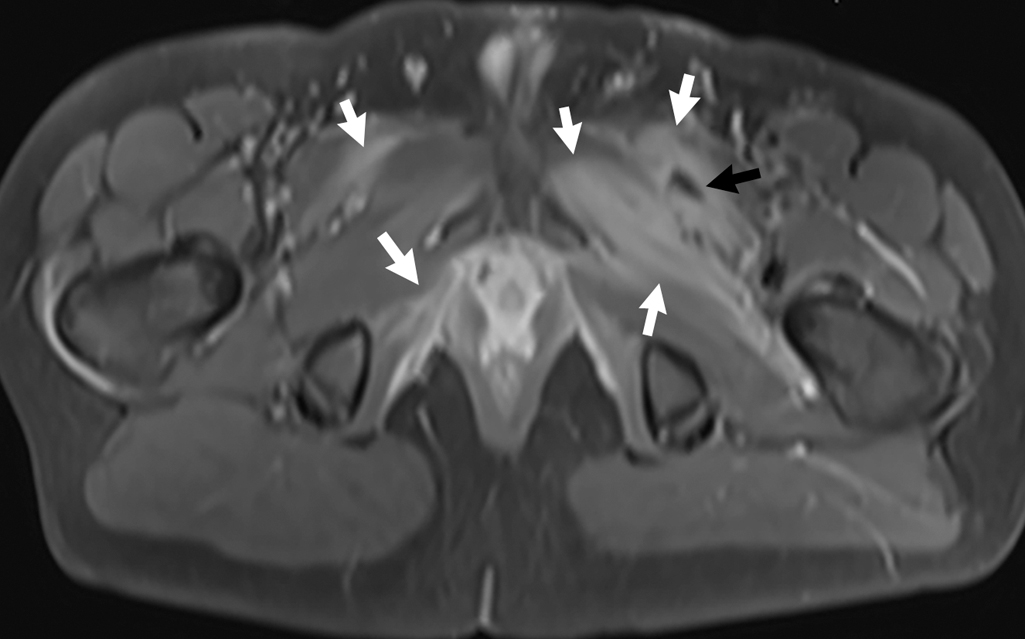
With the history, physical examination findings and laboratory results, and negative plain radiography evaluation, the decision was made to obtain MRI of the pelvis and femur, with and without intravenous contrast. Selected images from this study are provided. Findings of pyomyositis are noted, with muscular edema in pelvic musculature bilaterally, left greater than right, with a loculated fluid collection in the left pectineus muscle, most consistent with abscess ( Fig. 71.1 ). There is also bone marrow edema in the medial left acetabulum suggestive of osteomyelitis ( Figs. 71.2 and 71.3 ).