• Late-stage AIDS patients usually with CD4 < 100 cells/mm³
• Now considered rare condition due to HAART
• Patients present with RUQ pain, fever, weight loss, diarrhea, and markedly elevated alkaline phosphatase
• Primary treatment is reconstituting immune function using HAART, which can reverse cholangiopathy in some cases
(Left) Cholangiogram demonstrates a pruned appearance of the extrahepatic biliary tree with multiple beaded strictures, attributable in this case to AIDS cholangiopathy given the patient’s very low CD4 count.
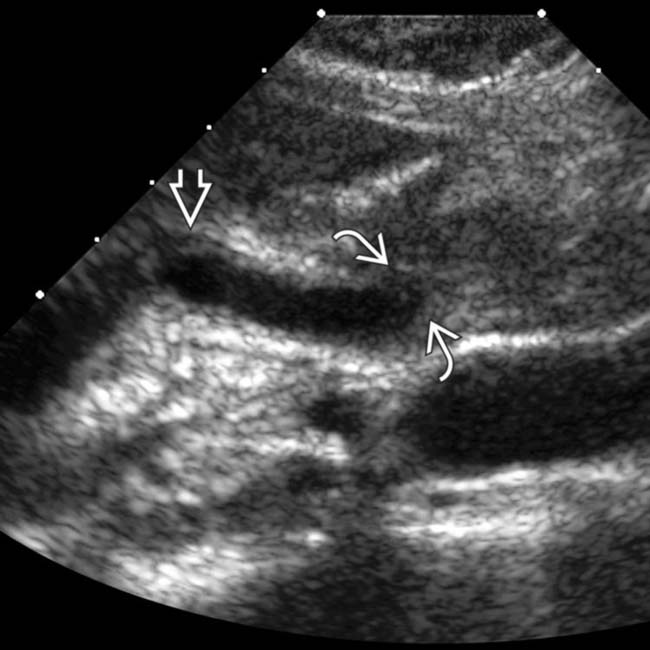
(Right) Ultrasound of the portal hepatis in a man with Cryptosporidium cholangitis shows tapered narrowing of a dilated distal common bile duct (CBD) and wall thickening . (Courtesy K. Hosseinzadeh, MD.)
(Left) ERCP shows abnormal intrahepatic ductal arborization, with foci of stricture, dilation, and abrupt termination of ducts. The common duct is dilated, and the distal duct is strictured . Intrahepatic biliary strictures in AIDS cholangitis can resemble those seen in PSC.
(Right) MRCP shows strictured intrahepatic ducts , extrahepatic biliary ductal dilatation, a narrowed distal CBD , and papillary stenosis . This combination is characteristic of AIDS cholangiopathy. (Courtesy V. Kabathina, MD.)
TERMINOLOGY
Synonyms
• AIDS- or HIV-related cholangitis, AIDS-related sclerosing cholangitis, AIDS-related cholangiopathy
Definitions
• Spectrum of biliary inflammation caused by AIDS-related opportunistic infections leading to biliary strictures/obstruction or acalculous cholecystitis
IMAGING
General Features
• Best diagnostic clue
AIDS patient, typically with a very low CD4 count (< 100/mm³) with multiple intrahepatic strictures, ampullary stenosis, or gallbladder (GB) wall thickening from cholecystitis
• ERCP: Papillary stenosis with proximal CBD dilation, CBD strictures/ulcerations, and multiple intrahepatic strictures
Combination of ampullary stenosis and intrahepatic strictures is unique to AIDS cholangiopathy
• ERCP is gold-standard for diagnosis but carries risks related to invasive procedure
CT Findings
• CECT
Dilatation of CBD with tapered narrowing of distal CBD
– ± thickening and hyperenhancement of CBD wall
Beaded appearance of intrahepatic ducts: Alternating sites of narrowing, normal ducts, and dilated ducts
Gallbladder (GB) wall thickening and pericholecystic fat stranding in patients with acalculous cholecystitis
MR Findings
• MR/MRCP very sensitive (85-100%) and specific (92-100%)
Allows visualization of proximal ducts even in setting of tight strictures (advantage over ERCP)
• Papillary stenosis with tapered narrowing of distal CBD (without abrupt margins) and proximal CBD dilatation
± long-segment extrahepatic bile duct strictures
– ± thickening and hyperenhancement of bile duct wall on T1WI C+ in setting of acute inflammation
Pancreatic duct usually normal in caliber
• Intrahepatic ductal strictures resembling PSC
Multifocal sites of alternating strictures, normal caliber ducts, and dilated ducts producing beaded appearance
Greater than expected visualization of intrahepatic ducts on MRCP should suggest intrahepatic strictures
• GB wall thickening and pericholecystic inflammatory changes in patients with acalculous cholecystitis
Ultrasonographic Findings
• Dilated intrahepatic ducts with CBD thickening and periductal hyper-/hypoechoic areas
Usually smooth tapered narrowing of distal CBD in setting of papillary stenosis
• Diffuse GB thickening ± sonographic Murphy sign in the setting of acalculous cholecystitis
Imaging Recommendations
• Best imaging tool
US: Screening modality for biliary ductal dilatation
MRCP: Best noninvasive modality
ERCP: Gold standard for establishing diagnosis and excluding malignancy at strictures using cytologic brushing
• Protocol advice
US protocol: Parasagittal view of CBD to demonstrate mural thickening
MRCP protocol: Axial and coronal single-shot fast spin-echo (SSFSE); obliques, heavily T2WI
DIFFERENTIAL DIAGNOSIS
Primary Sclerosing Cholangitis
• Chronic inflammatory disorder involving the intrahepatic and/or extrahepatic bile ducts
• Beaded and pruned appearance of intrahepatic ducts with asymmetric short segment strictures alternating with normal sized ducts and sites of saccular dilatation
Involvement of intrahepatic ducts is indistinguishable from AIDS cholangiopathy without clinical history
Only gold members can continue reading. Log In or Register to continue
 ± thickening and hyperenhancement of bile duct wall on T1WI C+ images in setting of acute inflammation
± thickening and hyperenhancement of bile duct wall on T1WI C+ images in setting of acute inflammation Beaded appearance of intrahepatic ducts with alternating strictures, normal ducts, and dilated ducts
Beaded appearance of intrahepatic ducts with alternating strictures, normal ducts, and dilated ducts



 and wall thickening
and wall thickening  . (Courtesy K. Hosseinzadeh, MD.)
. (Courtesy K. Hosseinzadeh, MD.)
 is dilated, and the distal duct is strictured
is dilated, and the distal duct is strictured  . Intrahepatic biliary strictures in AIDS cholangitis can resemble those seen in PSC.
. Intrahepatic biliary strictures in AIDS cholangitis can resemble those seen in PSC.
 , extrahepatic biliary ductal dilatation, a narrowed distal CBD
, extrahepatic biliary ductal dilatation, a narrowed distal CBD  , and papillary stenosis
, and papillary stenosis  . This combination is characteristic of AIDS cholangiopathy. (Courtesy V. Kabathina, MD.)
. This combination is characteristic of AIDS cholangiopathy. (Courtesy V. Kabathina, MD.)










 Multifocal sites of alternating strictures, normal caliber ducts, and dilated ducts producing beaded appearance
Multifocal sites of alternating strictures, normal caliber ducts, and dilated ducts producing beaded appearance






 Involvement of intrahepatic ducts is indistinguishable from AIDS cholangiopathy without clinical history
Involvement of intrahepatic ducts is indistinguishable from AIDS cholangiopathy without clinical history





