Case presentation
A 2-year-old male presents with acute right leg pain after falling while jumping on a trampoline. Apparently, he fell off the trampoline onto the ground and landed on his left leg. The distance was estimated at 3 ft (approximately 1 m) and the incident was witnessed by his parents and two older siblings. There is no reported loss of consciousness. The child is unable to ambulate secondary to pain. His vital signs are age appropriate except for a heart rate of 120 beats per minute. He is crying even before his examination from what appears to be left thigh pain. His physical examination shows no obvious injury, other than left thigh edema and he is tender on palpation. He has no neck or back pain. He is neurovascularly intact.
Imaging considerations
Children who sustain extremity injuries may need imaging. The decision to image is based on history and physical examination findings. Proper imaging technique is essential if imaging is employed.
Plain radiography
Plain radiography of the injured extremity is all that is generally required to properly evaluate the presence of fractures. A two-view study is preferred, consisting of anteroposterior (AP) and lateral views. Appropriate pain control is paramount in order to obtain clinically useful images of the injured extremity. The clinician should also consider imaging of the area above and below the involved bone if injury is suspected. For example in this child, consideration should be given to imaging the pelvis, lower extremity (tibia-fibula), ankle, and foot if clinically indicated. There are times when a complete imaging series is not practical (e.g., deformity preventing full range of motion and positioning for two views). In these situations, a single AP view will suffice. Of particular concern are patients with neurovascular compromise; do not delay treatment in these patients to obtain imaging. Once the situation has stabilized, appropriate imaging studies can be obtained.
Computed tomography (CT)
Ipsilateral femoral neck fractures are associated with adult femoral shaft fractures in up to 9% of patients, prompting utilization of CT to detect these fractures. However, in the pediatric population, this association is quite low. In pediatric patients, routine CT imaging to look for associated femoral neck fracture with femoral shaft fractures is not recommended. CT utilization should be based on clinical examination and mechanism of injury, as well as concern for other injuries.
Imaging findings
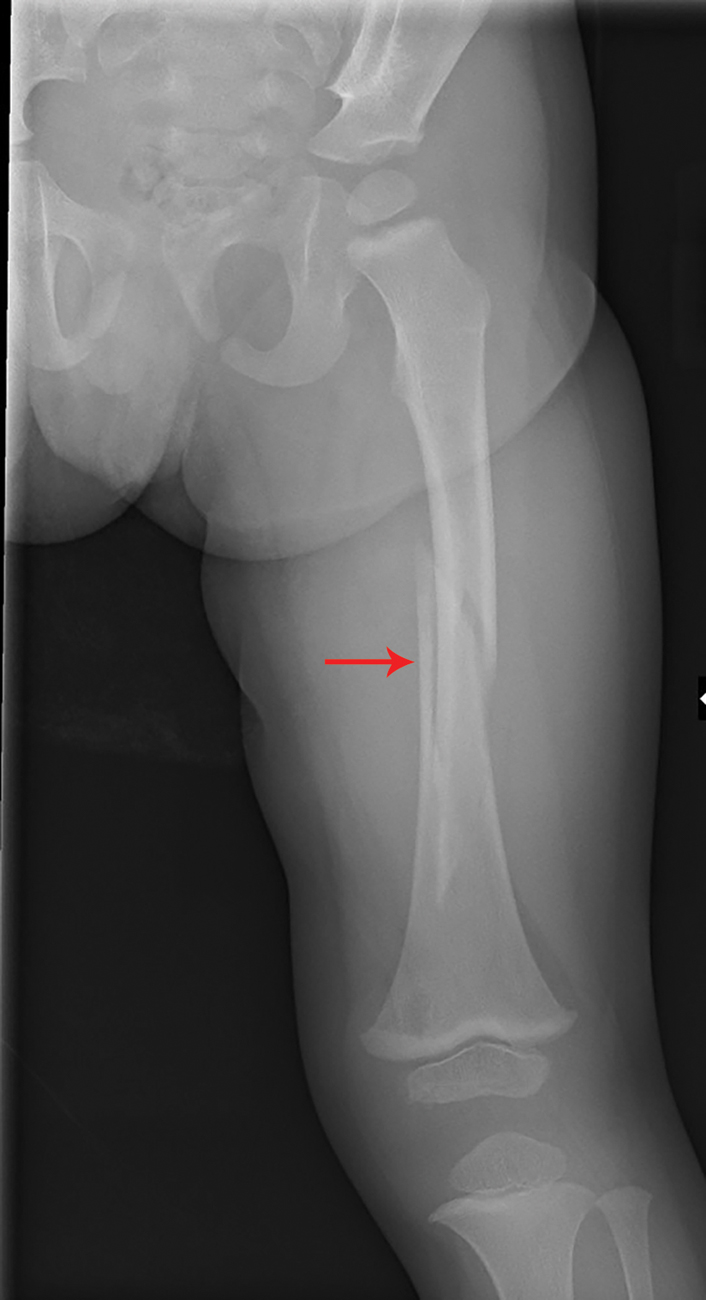
This child had a two-view study of the injured leg. There is a spiral, mid to distal diaphyseal femur fracture with minimal degree of displacement of the distal fragment ( Figs. 64.1 and 64.2 ). The second set of images shows a nondisplaced, oblique distal femur metaphyseal fracture in a different patient, extending toward the physis, consistent with a Salter-Harris type II fracture ( Figs. 64.3 and 64.4 ).