a precursor of subluxation and dislocation of the hip, although some authorities use the term developmental dysplasia of the hip (DDH) to denote all stages of CDH. In congenital subluxation of the hip, there is an abnormal relationship between the femoral head and the acetabulum, but the two are in contact (Fig. 32.7). Congenital dislocation of the hip, however, is marked by the femoral head’s complete loss of contact with the acetabular cartilage; the proximal femur is displaced most often superiorly, but lateral, posterior, and posterolateral dislocation may also be seen (Fig. 32.8).
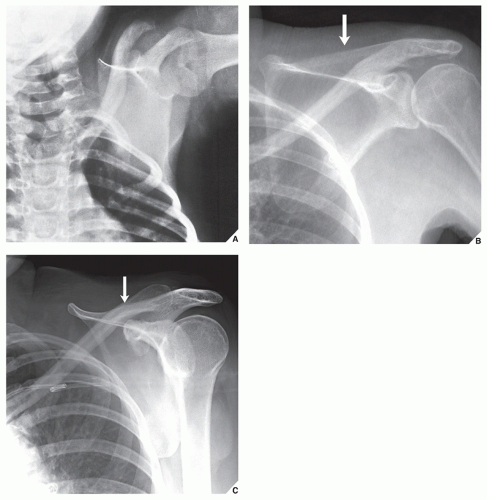 FIGURE 32.1 Sprengel deformity. (A) Anteroposterior radiograph of the left shoulder of a 1-year-old boy demonstrates a high position of the left scapula typical of Sprengel deformity. (B) Anteroposterior and (C) oblique radiographs of the left shoulder of a 58-year-old woman, who remembers having “a crooked shoulder blade” since early childhood, show congenital elevation of the left scapula (arrows). |
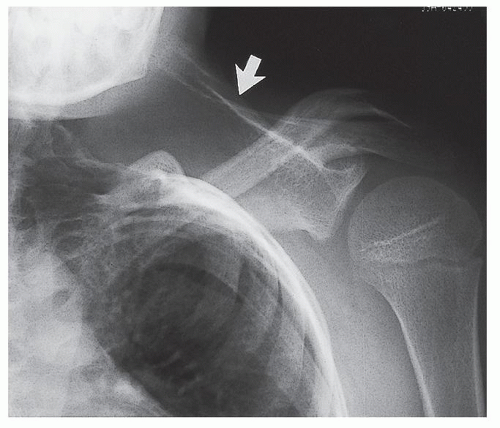 FIGURE 32.2 Klippel-Feil syndrome and Sprengel deformity. Anteroposterior radiograph of the left shoulder of a 13-year-old boy with Klippel-Feil syndrome shows an elevated scapula (arrow). |
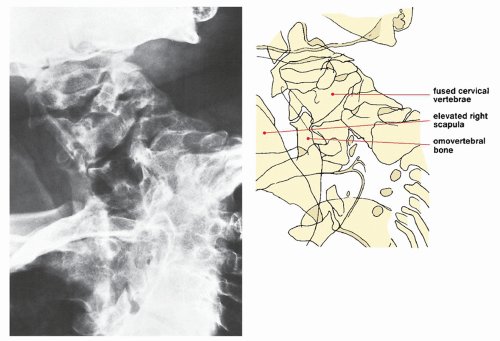 FIGURE 32.3 Klippel-Feil syndrome and Sprengel deformity. Posteroanterior radiograph of the cervical and upper thoracic spine in a 37-year-old woman with Sprengel deformity associated with Klippel-Feil syndrome (fusion of the cervical vertebrae) shows the omovertebral bone connecting the elevated right scapula and the C5 vertebra. |
TABLE 32.1 Radiographic Criteria for the Diagnosis of Madelung Deformity | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
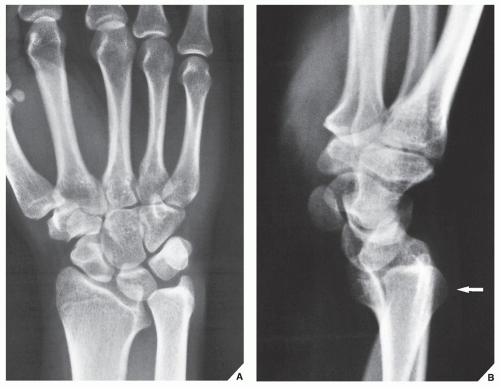 FIGURE 32.4 Madelung deformity. (A) Posteroanterior radiograph of the left wrist of a 21-year-old woman shows a decrease in the length of the radius, the distal end of which has assumed a triangular shape. This is associated with a triangular configuration of the carpus, with the lunate at the apex wedged between the radius and the ulna. (B) Lateral radiograph demonstrates dorsal subluxation of the ulna (arrow). |
 FIGURE 32.5 Madelung deformity. (A) Posteroanterior and (B) lateral radiographs of the left wrist of a 42-year-old woman show characteristic changes of this anomaly including decreased length of the radius, elongation of the ulna associated with dorsal subluxation, and triangular configuration of the carpus with lunate wedged between the radius and the ulna. (Courtesy of Robert M. Szabo, MD, Sacramento, California). |
TABLE 32.2 Most Effective Radiographic Projections and Radiologic Techniques for Evaluating Common Anomalies of the Pelvic Girdle and Hip | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 32.3 Clinical Manifestations of Congenital Dislocation of the Hip | ||
|---|---|---|
|
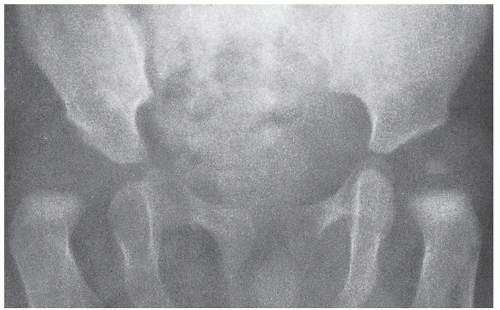 FIGURE 32.6 Congenital hip dysplasia. Anteroposterior radiograph of the pelvis of a 1-year-old boy shows a slightly flattened acetabulum and delayed appearance of the ossification center for the right femoral epiphysis; that of the left epiphysis is normally centered over the triradiate cartilage. |
 FIGURE 32.7 Congenital hip dysplasia. Anteroposterior radiograph of the pelvis of a 1-year-old girl shows congenital superolateral subluxation of the left hip. Note the slightly smaller size of the left femoral epiphysis. |
The Hilgenreiner line or Y-line, which is drawn through the superior part of the triradiate cartilage, is itself a valuable indicator of femoroacetabular relations and serves as the basis for all other indicators.
The acetabular index, which is an angle formed by a line tangent to the acetabular roof and the Y-line, cannot alone be diagnostic of dislocation because it can occasionally exceed 30 degrees in normal subjects. Generally, however, values greater than 30 degrees are considered abnormal and indicate impending dislocation. Some investigators propose that only angles in excess of 40 degrees are significant.
The Perkins-Ombredanne line, which is drawn perpendicular to the Y-line through the most lateral edge of the ossified acetabular cartilage, is helpful in determining subluxation and dislocation of the hip. The intersection of this line with the Y-line creates four quadrants; normally, the medial aspect of the femoral neck or the ossified capital femoral epiphysis falls in the lower medial quadrant.
The Shenton-Menard line, which forms a smooth arc through the medial aspect of the femoral neck and the superior border of the obturator foramen, may be interrupted in subluxation or dislocation of the hip. Even under normal circumstances, however, the arc may not be smooth if the radiograph is obtained with the hip in external rotation and adduction.
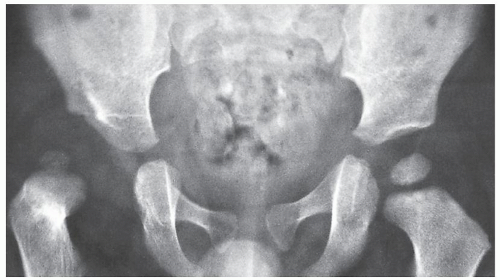
FIGURE 32.8 Congenital hip dislocation. Anteroposterior radiograph of the pelvis of a 2-year-old boy demonstrates complete superolateral dislocation of the right hip. Note the abnormal position of the center of ossification in relation to the acetabulum compared with the normal left hip.
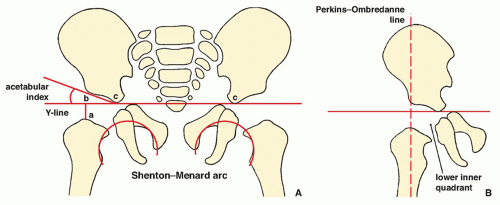
FIGURE 32.9 Measurements helpful to evaluate the relation of the femoral head to the acetabulum. (A) The Hilgenreiner line or Y-line is drawn through the superior part of the triradiate cartilage. In normal infants, the distance represented by a line (ab) perpendicular to the Y-line at the most proximal point of the femoral neck should be equal on both sides of the pelvis, as should the distance represented by a line (bc) drawn coincident with the Y-line medially to the acetabular floor. In infants aged 6 to 7 months, the mean value for the distance (ab) has been determined to be 19.3 ± 1.5 mm; the distance for (bc) is 18.2 ± 1.4 mm. The acetabular index is an angle formed by a line drawn tangent to the acetabular roof from point (c) at the acetabular floor on the Y-line. The normal value of this angle ranges from 25 to 29 degrees. The Shenton-Menard line is an arc running through the medial aspect of the femoral neck and the superior border of the obturator foramen. It should be smooth and unbroken. (B) The Perkins-Ombredanne line is drawn perpendicular to the Y-line through the most lateral edge of the ossified acetabular cartilage, which actually corresponds to the anteroinferior iliac spine. In normal newborns and infants, the medial aspect of the femoral neck or the ossified capital femoral epiphysis falls in the lower inner quadrant. The appearance of either of these structures in the lower outer or upper outer quadrant indicates subluxation or dislocation of the hip.
The Andrén-von Rosen line, which is drawn on a radiograph obtained with the hips abducted 45 degrees and internally rotated, describes the relation of the longitudinal axis of the femoral shaft to the acetabulum (Fig. 32.10). In dislocation or subluxation of the hip, this line bisects or falls above the anterosuperior iliac spine.
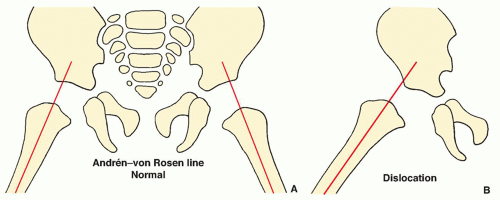 FIGURE 32.10 The Andrén-von Rosen line. (A) With at least 45 degrees of hip abduction and internal rotation, the line is drawn along the longitudinal axis of the femoral shaft. In normal hips, it intersects the pelvis at the upper edge of the acetabulum. (B) In subluxation or dislocation of the hip, the line bisects or falls above the anterosuperior iliac spine. |
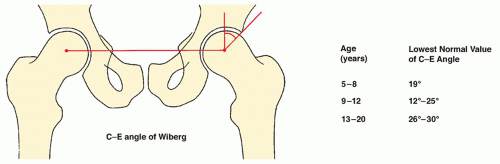 FIGURE 32.11 Angle of Wiberg. The C-E angle of Wiberg is helpful in evaluating the development of the acetabulum and its relation to the femoral head. A baseline is projected, connecting the centers of the femoral heads. The C-E angle is formed by two lines originating in the center of the femoral head, one drawn perpendicular to the baseline into the acetabulum, and the other connecting the center of the femoral head with the superior acetabular lip. Values below the lowest normal value given for each age group indicate hip dysplasia. |
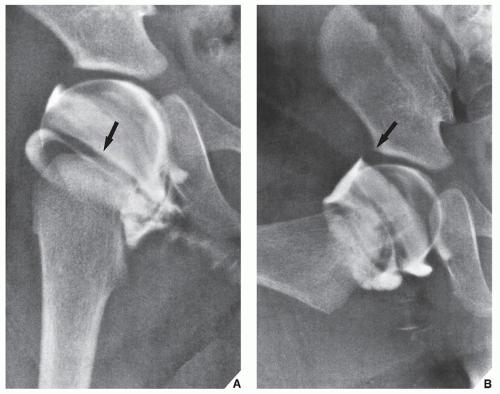 FIGURE 32.12 Arthrogram of a normal hip. (A) Arthrogram of the right hip in the neutral position in a 5-month-old boy shows contrast agent accumulating in the large recesses medial and lateral to the constriction produced by the orbicular ligament (arrow). Note the smoothness and even thickness of the cartilage covering the femoral head. (B) On the frog-lateral view, contrast is seen outlining the edge of the cartilaginous labrum (arrow). The ligamentum teres can be seen medial to the femoral head, extending from the inferior portion of the acetabulum. |
 FIGURE 32.13 Arthrogram of congenital hip dysplasia. (A) Arthrogram of the right hip in the neutral position in a 1-year-old girl with congenital subluxation of the hip shows the typical displacement of the hip lateral to but below the acetabular labrum. There is accumulation of contrast agent in the stretched capsule (arrow), and the ligamentum teres is elongated. (B) In the frog-lateral position, the head moves more deeply into the acetabulum, but subluxation is still present. |
 FIGURE 32.14 Arthrogram of congenital hip dislocation. (A) Anteroposterior radiograph of the right hip in an 8-year-old girl demonstrates complete superolateral dislocation of the femoral head. Note the shallow acetabulum. (B) Arthrogram of the hip shows a deformed cartilaginous limbus and stretching of the ligamentum teres. The femoral head lies superior and lateral to the edge of the cartilaginous labrum. Note the accumulation of contrast agent in the loose joint capsule. |
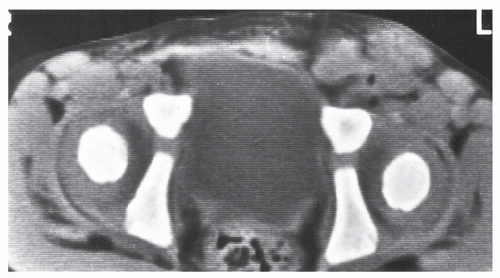 FIGURE 32.15 CT of the normal hips. Axial section of both hips in a 19-monthold infant shows good congruity of the acetabula and femoral heads, which are centered over the triradiate cartilage. |
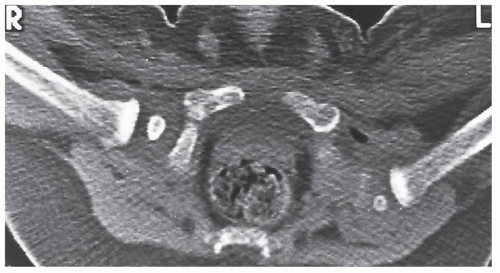 FIGURE 32.16 CT of congenital hip dislocation. Axial section through the proximal femora and hips of a 6-month-old boy shows posterolateral dislocation of the left hip. The right hip is normal. |
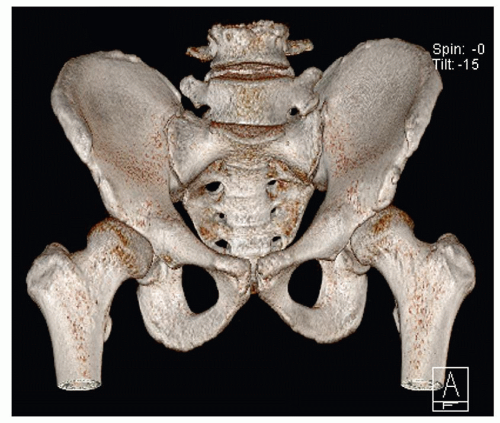 FIGURE 32.17 3D CT of congenital hip dysplasia. 3D reconstructed CT image of the pelvis of a 32-year-old man with congenital bilateral hip dysplasia shows undercoverage of the femoral heads by bony acetabula. |
in the triradiate cartilage and when growth remains for remodeling of the joint surfaces. Steele triple innominate osteotomy is usually indicated for children older than age 6 to 8 years who have an immobile symphysis pubis. In addition to Salter osteotomy, osteotomies of the inferior and superior pubic rami are performed. The acetabulum is brought forward and rotated in the frontal plane, avoiding external rotation. The Chiari pelvic osteotomy is usually reserved for older children. This is a displacement osteotomy that essentially provides a shelf or buttress to limit further proximal subluxation of the femoral head. This procedure displaces the femoral head medially and increases the weight-bearing surface of the head by producing an overhanging superior acetabular ledge. This technique may also be combined with a varus derotational osteotomy of the femoral neck. Ganz osteotomy, also known as Bernese periacetabular osteotomy, is usually performed in older children and adolescents and occasionally in adults. The principle behind the procedure is to allow anterior and lateral rotation and medialization of the hip without violation of the posterior column of the hemipelvis. Osteotomies are performed around the acetabulum (complete osteotomy of the pubis and biplanar osteotomy of the ilium); however, the cut through the posterior column of the ischium is incomplete. The acetabular fragment is rotated anteriorly and laterally (maintaining anteversion) and is then medialized. This procedure provides excellent femoral head coverage and acetabular mobility.
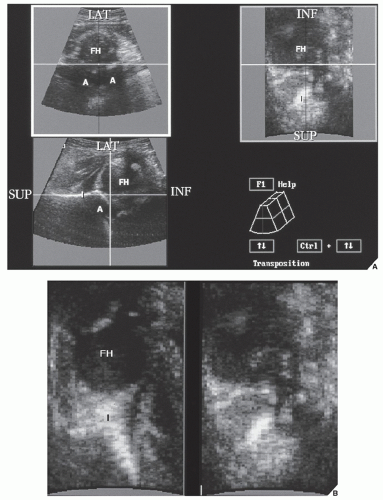 FIGURE 32.18 Ultrasound of congenital hip dysplasia. (A) On the coronal 3D ultrasound image of the left hip in a 3-day-old girl (lower left) the acetabulum (A) appears shallow, and subluxation of the femoral head can be observed at the intersection of the ilium (I) line with the medial third of the femoral head (FH). On the reconstructed axial image (upper left), the femoral head is subluxated but still in contact with the acetabulum. On the sagittal image (upper right), only the peripheral segment of femoral head is visualized. (B) A sagittal image of a normal left hip (left) is shown for comparison. Note that femoral head (FH) is centered over the ilium line (I). A sagittal image of a subluxated head (right) clearly shows distortion of femoral head-ilium line relationship. LAT, lateral; INF, inferior; SUP, superior. (From Gerscovich EO, Greenspan A, Cronan MS, Karol LA, McGahan JP. Three-dimensional sonographic evaluation of developmental dysplasia of the hip: preliminary findings. Radiology 1994;190:407-410.) |
 FIGURE 32.19 3D ultrasound of congenital hip dysplasia. (A) Craniocaudal projection (bird’s eye view) of a normal left hip shows the ilium (I) projecting over the midportion of the femoral head (FH) (arrows outline its contour). (B) Craniocaudal projection of a subluxated left hip shows that the ilium (I) projects over the medial portion of the femoral head (FH) (arrows outline its contour). The femoral head is laterally displaced. LAT, lateral; ANT, anterior; POST, posterior. (From Gerscovich EO, Greenspan A, Cronan MS, Karol LA, McGahan JP. Three-dimensional sonographic evaluation of developmental dysplasia of the hip: preliminary findings. Radiology 1994;190:407-410.) |
 FIGURE 32.20 MRI of congenital hip dysplasia. (A) Coronal T2-weighted MRI of a 5-year-old boy with left DDH demonstrates a shallow left acetabulum, uncoverage of the femoral head, and a superiorly rotated and torn labrum (arrow). (B) Coronal T1-weighted MRI of a 5-month-old boy with left DDH demonstrates lateral subluxation and uncoverage of the femoral head, a dysplastic and shallow acetabulum, an everted and hypertrophied labrum (arrow), and hypertrophy of the pulvinar and transverse ligament (arrowheads). |
 FIGURE 32.21 Treatment of congenital hip dysplasia. (A) Anteroposterior radiograph of the pelvis in a 1-year-old boy demonstrates the typical appearance of congenital dislocation of the left hip. (B) After conservative treatment with a Pavlik harness at age 2 years, there is still subluxation. Note the broken Shenton-Menard arc. At age 3 years, after further conservative treatment by skin traction and application of a spica cast, there is almost complete reduction of subluxation, as demonstrated by contrast arthrography (C). (D) CT scan, however, demonstrates some minimal residual lateral displacement of the femoral head, as evidenced by the medial accumulation of contrast. |
 FIGURE 32.22 The Gage and Winter system. This measurement of stations for monitoring the progress of treatment by traction and the descent of the femoral head is based on the position of the proximal femoral metaphysis relative to the ipsilateral acetabulum and the contralateral normal hip. |
 FIGURE 32.23 Femoral varus derotational osteotomy and acetabular shelf procedure. (A) Anteroposterior radiograph of the left hip demonstrates a bone allograft attached with two metallic screws in the superior lateral aspect of a dysplastic left acetabulum (arrow), providing good coverage of the femoral head (arrowhead). Note the hardware of the varus derotational osteotomy in the proximal left femur. (B) Coronal T2-weighted MRI of the same patient demonstrates the artifact due to the screws used for the shelf operation (long arrow). The humeral head is still separated from the acetabulum (short arrow) due to the presence of infolded labrum (arrowhead). Compare with the right side for the normal position of the femoral head within the acetabulum. |
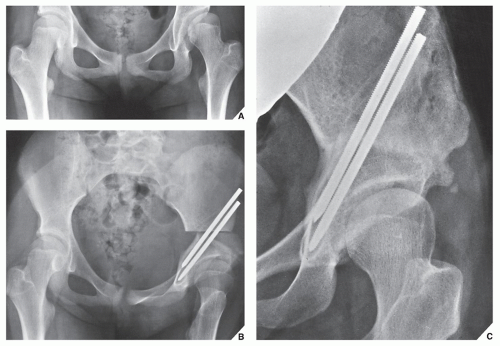 FIGURE 32.24 Salter osteotomy. (A) Anteroposterior radiograph of the pelvis in a 7-year-old girl with CDH shows persistent superolateral subluxation of the left hip following conservative treatment. Note the anterolateral orientation of the acetabulum in comparison with the normal right hip. (B) Postoperative film after Salter osteotomy through the supraacetabular portion of the iliac bone shows the acetabulum displaced anterolaterally and downward; a triangular bone graft, taken from the anterolateral aspect of the ilium, is secured by two Steinmann pins at the site of the osteotomy. (C) Four years later, the femoral head is completely covered by the acetabulum. Because of a valgus configuration of the femoral neck, the patient may yet require a varus derotational osteotomy. |
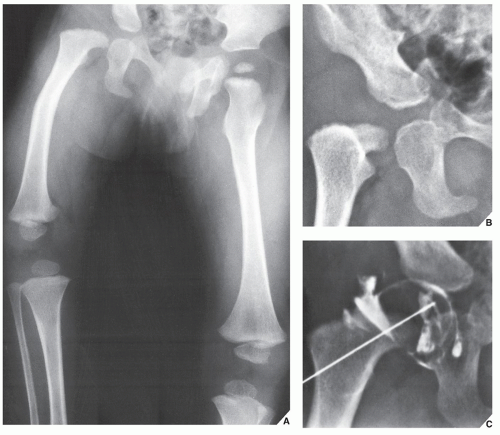 FIGURE 32.25 Proximal femoral focal deficiency. (A) Anteroposterior radiograph in an 18-month-old boy who had a short right leg demonstrates a varus configuration at the right hip joint, the absence of an ossification center for the proximal femoral epiphysis, and shortening of the femur—the classic radiographic features of PFFD. (B) A coned-down view of the right hip shows superior, posterior, and lateral displacement of the proximal femoral segment in relation to the acetabulum. (C) Arthrography was performed to classify the abnormality, and the presence of the femoral head in the acetabulum and the absence of any defect in the femoral neck were found, making this a type A focal deficiency. |
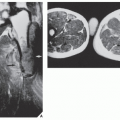
 FIGURE 32.26 MRI of proximal focal femoral deficiency. Coronal T1-weighted image of a young girl with PFFD demonstrates absent proximal right femoral shaft terminating in a blunted chondral surface (arrow), which was not bridging with the hypoplastic proximal femoral head and neck (not shown). |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


