(1)
Department of Radiology, Saitama Medical University, Moroyama, Saitama, Japan
Abstract
ACL is an intra-articular extrasynovial structure.
3.1 Anatomy
ACL is an intra-articular extrasynovial structure.
Its mean length is 38 mm and width is 11 mm. Its fibers run in a spiral fashion for the entire length.
Volume of ACL is larger in men than women, in proportion to the difference in height.
ACL has two main fiber bundles: anteromedial bundle (AMB) and posterolateral bundle (PLB) (Fig. 3.1). On MRI, it may occasionally be possible to differentiate these two bundles (Fig. 3.2).
Fig. 3.1
Two fiber bundles of ACL. The anteromedial bundle (AMB) forms the anterior portion of the ACL, while the posterolateral bundle (PLB) forms the posterior portion. Overall, ACL is subject to the maximum tension at the maximum extension and 90-degree flexion, and the tension mainly acts on the AMB, resulting in frequent injury of AMB (Figure modified from Girgis et al. 1975)
Fig. 3.2
Two fiber bundles of ACL on MRI. AMB (arrows) and PLB (arrowheads) can sometimes be differentiated on MRI. These bundles spread out at the tibial attachment site, but the fibers run in a spiral fashion and may appear as one bundle at the femoral attachment site
AMB forms the anterior border of the ACL, and it is easily visualized in sagittal images and also easily damaged.
ACL runs diagonally from intercondylar region of the femur from posterolateral to anteromedial direction.
ACL will be subject to the maximum tension at maximum extension and at 90-degree flexion. This tension mainly acts on AMB. At 45-degree flexion, ACL becomes slightly relax.
Femoral attachment of the ACL is approximately 23 mm long, which is smaller than tibial attachment site, making it more vulnerable to injury. About 80% of ACL damage in skiing injury occurs at the femoral attachment site (Fig. 3.3a).
Fig. 3.3
ACL of the cadaveric knee. (a) Extended and (b) lightly flexed cadaveric knee joint. ACL is a ligament that runs diagonally within the intercondylar space. At the femoral attachment site, peripheral portion of the fiber bundle attaches to the medial surface of the lateral femoral condyle, in a fanlike fashion (a, arrows). When the knee is flexed, ACL becomes distant from the ceiling of the intercondylar space, and it appears thicker, making it easier for us to visualize it in the sagittal MRI (b)
ACL attaches to the tibia at the site spreading like a fan between the tibial spine and the anterior horn of the medial meniscus. The length of the attachment site is on average 30 mm (i.e., larger than that at the femoral attachment, Fig. 3.4).
Fig. 3.4
Tibialattachment site of the ACL. (a) Cadaveric knee and (b) PDWI of a human subject. ACL attaches to the tibia at the site spreading like a fan between the tibial spine and the anterior horn of the medial meniscus (arrows). This configuration enables a firm attachment
References
Fayad LM, Rosenthal EH, Morrison WB, Carrino JA. Anterior cruciate ligament volume: analysis of gender differences. J Magn Reson Imaging. 2008;27:218–23.
Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;106:216–31.
Kennedy JC, Weinberg HW, Wilson AS. The anatomy and function of the anterior cruciate ligament. J Bone Joint Surg. 1974;56-A:223–35.
3.2 Image Acquisition
Most vendors supply a dedicated cylindrical knee coil.
When the knee is imaged using the cylindrical knee coil, the knee tends to be fixed in an extended position (Fig. 3.5a).
Fig. 3.5
(a) Cylindrical knee coil with an ankle holder. Most vendors supply a cylindrical knee coil with an ankle holder. Using these by following manufacturer’s user instruction, the knee tends to be fixed at an extended position. (b) Cylindrical knee coil with a small knee pad. A small pad is placed in the popliteal fossa (arrow), and the ankle holder is removed. The knee is now flexed by 15°
If the sagittal images of the extended knee is acquired:
1.
The anterior border of the ACL will be in touch with the ceiling of the intercondylar space, making it difficult to grasp the overall picture of the ACL. This is an important issue because AMB forms the anterior portion of the ACL and is vulnerable to injury.
2.
Visualization of the femoral attachment site of the ACL becomes unclear due to partial volume effect between ACL and the medial surface of the lateral femoral condyle.
3.
Intrasubstance hyperintensity is often observed within ACL, and this is thought to be due to magic angle effect (see Chap. 2).
By using a pad or other supporting objects, the knee can be fixed at max 30° (average 15°) of flexion while using the knee coil inside the superconducting magnet (Fig. 3.5b).
When the knee is lightly flexed, ACL becomes distant from the ceiling of the intercondylar space, and it appears thicker, making it easier for us to visualize it in the sagittal MRI. The flexed position also enables clearer visualization of the femoral attachment site of ACL (Fig. 3.6).
Fig. 3.6
Differences of ACL appearance when the knee is extended and flexed as shown in Fig.3.5. (a) Knee was fixed in an extended position, corresponding to the Fig. 3.5a. (b) Knee was fixed in a flexed position, corresponding to the Fig. 3.5b. When the knee is lightly flexed, ACL becomes distant from the ceiling of the intercondylar space, and it appears thicker, making it easier for us to visualize it in the sagittal MRI. The flexed position also enables clearer visualization of the femoral attachment site of ACL (arrows)
In analogy, the ACL looks like a flat tape at the femoral attachment site, but as it becomes more distant from the ceiling of the intercondylar space, it becomes like a rope as the fibers are twisted around the longitudinal axis. This is why visualization of ACL in sagittal MRI becomes easier when the knee is slightly flexed.
Slight knee flexion does not adversely affect the visualization of PCL or menisci.
Reference
Niitsu M, Ikeda K, Fukubayashi T, et al. Knee extension and flexion: MR delineation of normal and torn anterior cruciate ligaments. J Comput Assist Tomogr. 1996;20:322–7.
3.2.1 Appropriate Clothes for MRI Examination
Stockings or socks covering the knee should be removed because they can lower the image quality.
A “pants-style” examination costume should be used so that the cables from coil do not touch the patient’s skin to cause burns.
Dignity should be preserved during examination (especially female patients).
3.3 MRI Findings of Normal ACL
ACL runs within the intercondylar space between the femoral and tibial attachment sites in a curved fashion.
In sagittal images, the anterior border of the ACL is smooth and shows hypointensity in all sequences (Fig. 3.7). This corresponds to the fibers of AMB. The middle and posterior portion of the ACL may show mild hyperintensity due to some fat tissue that is present within the ACL fibers, which is less dense at these locations compared to the anterior portion.
Fig. 3.7
Normal ACL. PDWI (left, SE 2,000/20) and T2WI (right, SE 2,000/60) of the knee. In sagittal images, the anterior border of the ACL is smooth and shows hypointensity in all sequences. This corresponds to the fibers of AMB. The middle and posterior portion of the ACL may show mild hyperintensity due to some fat tissue (arrow) that is present within the ACL fibers
ACL tends to appear generally more hyperintense than PCL.
3.4 Characteristics of ACL Tear
ACL tear is common ligamentous tear.
This is due to the fact that ACL is more vulnerable to injury than PCL due to thinner fiber bundles and a smaller attachment.
Women are 4–8 times more likely to sustain ACL tear than men, and an association with female sex hormone has been suggested.
In a typical scenario, a patient feels a “pop,” and a rapidly enlarging hematoma is seen. 60–80% of hemarthrosis of the knee coexists with ACL tear. If there is a fracture, fat droplets can also be seen within the hematoma.
ACL tear may have already been clinically diagnosed before MRI examination, but clinical symptoms associated with ACL tear can be variable.
References
Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;106:216–31.
Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield ML. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am J Sports Med. 1998;26:614–9.
3.4.1 Causes of ACL Tear
Commonly occurs following sports injuries
Knee flexion, valgus injury, and lateral rotation of the distal lower limb (e.g., skiing accident)
Overextension of the knee
Stopping or jumping while the knee is slightly flexed (e.g., characteristic to basketball and volley ball and more common in female athletes)
3.5 Complete Tear of ACL
Complete tear of all fibers of the ACL.
Approximately 70% occurs at the central portion of the ACL (Fig. 3.8). Approximately 20% occurs at the femoral attachment site (Fig. 3.9).
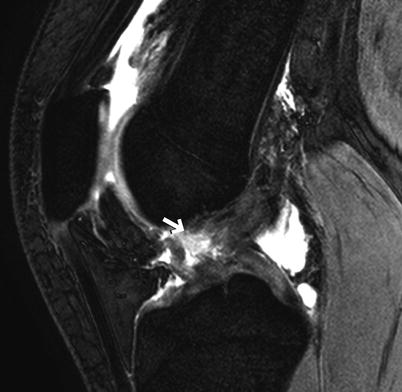
Fig. 3.8
Complete tear of ACL at the central portion. T2*WI of a teenage man. A complete loss of continuity of ACL at the central portion (arrow)
Fig. 3.9
Complete tear of the ACL at the femoral attachment site. (a) PDWI and (b) axial FS PDWI of a man in his forties. ACL has lost its continuity at the femoral attachment site (arrow). It is important to confirm this in all three planes (i.e., sagittal, coronal, and axial, arrowhead)
Complete tear at the tibial attachment site is rare.
MRI findings
Discontinuation of ACL fibers.
It is relatively easy to diagnose a complete tear on MRI (sensitivity >90%).
3.6 Partial Tear of ACL
Partial tear of ACL occurs if only AMB or PMB, either entirely or partially, is torn. However, it is difficult differentiate these two bundles on MRI, and clinically all tears that are not complete are classified as partial tear.
Diagnosing partial tear of ACL on MRI is said to be very difficult.
AMB is more commonly affected than the PMB.
References
Yamato M, Yamagishi T. Can MRI distinguish between acute partial and complete anterior cruciate ligament tear? Nippon Acta Radiol. 1996;56:385–9.
Roychowdhury S, Fitzgerald SW, SOnin AH, Peduto AJ, Miller FH, Hoff FL. Using MR imaging to diagnose partial tears of the anterior cruciate ligament: value of axial images. AJR. 1997;168:1487–91.
MRI findings
Fibers may appear continuous.
Fine intrasubstance hyperintensity within the ACL or angulation of the ligament may be seen.
Immediately following an acute injury, edema, hemorrhage, and synovial thickening may hinder the imaging diagnosis, making it difficult to differentiate between partial and complete tear.
Pearls
Fix the knee in a slightly flexed position, as described earlier, to better delineate the anterior border of the ACL (Fig. 3.10)
Fig. 3.10
Partial tear of ACL. (a) PDWI, (b) coronal T2*WI, and (c) axial T2WI of the knee in a man in his 50s. The sagittal image shows the ACL at the femoral attachment site is not clearly delineated (arrow), which is suspicious for ACL tear, but it is difficult to confirm the diagnosis with this image alone. Looking at the cross-section of the ACL on both coronal and axial images reveal a localized hyperintensity within the ACL at the femoral attachment site (arrowhead, b and c), confirming the diagnosis of partial ACL tear
Acquire images which are as thin as possible and with highest possible anatomical resolution
3.6.1 Importance of Knee Positioning
It is essential to lightly flex the knee to better delineate the ACL when using a cylindrical knee coil. Place a pad in the popliteal fossa so that the distal lower limb does not move while scanning. If the padding is too little, the image will be affected by motion artifact, and if there is too much padding, the patient will complain of pain after about 20 min, resulting in suspension of the scanning. It is necessary to explain to the patient that their cooperation (i.e., not to move) is of paramount importance and ensure to talk to the patient during the scanning session for patients who are of nervous predisposition. If fat suppression is to be applied, pads that can compensate for magnetic field inhomogeneity should be used and try to position the coil in the center of the magnetic field as much as possible. In any case, the pre-imaging preparation and knee positioning are very important.
3.7 Acute Tear of ACL
Definition: “Acute” tear means that less than 2 weeks has passed since the time of injury.
MRI findings
ACL appears swollen and discontinuous (Fig. 3.11).

Fig. 3.11
Acute tear of ACL. T2*WI of a teenage man. ACL appears discontinuous and appear swollen for its entire length (arrows)
Intraligamentous linear hyperintensity is said to represent interstitial tear.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree