Strictures long and smooth without irregularity and may cause proximal biliary dilatation
• MR: MRCP images nicely demonstrate irregularity and strictures of intrahepatic or extrahepatic bile ducts (most commonly affecting distal CBD)
Affected segments demonstrate concentric ductal wall thickening with hyperenhancement on T1WI C+
Stricture long and smooth (without irregularity)
Findings of concomitant autoimmune pancreatitis
– Enlarged pancreas with abnormal signal (hypointense on T1WI and hyperintense on T2WI)
– Rim of peripheral hypoenhancement and low T2WI signal with delayed enhancement
– Multiple discontiguous pancreatic duct strictures on MRCP, which may resolve after administration of secretin
• CT: Circumferential focal or diffuse bile duct wall thickening with hyperenhancement of affected segments
PATHOLOGY
• Frequently associated with imaging findings of autoimmune pancreatitis and other manifestations of IgG4-related sclerosing disease
• Exact pathophysiology not well understood, but some evidence for both autoimmune and allergic mechanisms
CLINICAL ISSUES
• Typically affects middle-aged and elderly males
• Diagnosis based on a combination of imaging, histopathology, serologic (↑ IgG4) markers and clinical response to steroids/azathioprine
• May improve spontaneously, progress, or relapse, although relapse rate after therapy may be high (> 50%)
• Treatment with steroids typically effective, although other immunomodulators utilized in refractory cases
(Left) CECT of a jaundiced patient shows a thickened, slightly dilated common bile duct (CBD) and an enlarged, sausage-shaped pancreas . The appearance of the pancreas is consistent with autoimmune pancreatitis (AIP), and an elevated IgG4 indicates that the bile duct thickening is due to IgG4-related sclerosing cholangitis (ISC).
(Right) ERCP in same patient shows a stricture of the distal CBD, the most common manifestation of ISC. ISC and AIP resolved after steroid and azathioprine therapy.
(Left) Coronal CECT in a patient with known autoimmune pancreatitis (not shown) demonstrates tapered narrowing of the distal CBD with wall hyperenhancement, compatible with autoimmune cholangitis.
(Right) Coronal CECT in a patient with known autoimmune pancreatitis demonstrates wall thickening, hyperenhancement, and narrowing of the CBD with proximal biliary dilatation , in keeping with IgG4-related cholangitis.
• IRSD: Spectrum of disorders characterized by tumor-like lymphoplasmacytic infiltration and varying degrees of fibrosis in different organs
Pancreas is most commonly affected organ (autoimmune pancreatitis) followed by salivary glands and biliary tree
• ISC: Biliary manifestations of IRSD frequently associated with autoimmune pancreatitis (AIP)
Manifested as wall thickening and biliary strictures
IMAGING
General Features
• Best diagnostic clue
Bile duct wall thickening and strictures in setting of autoimmune pancreatitis
• Location
ISC classified based upon stricture location
– Type 1: Distal (intrapancreatic) common bile duct (CBD)
Most common type: May mimic pancreatic adenocarcinoma or cholangiocarcinoma
– Type 2: Strictures distributed throughout intra- and extrahepatic ducts
May mimic primary sclerosing cholangitis
– Type 3: Strictures of duct bifurcation and distal duct
May mimic cholangiocarcinoma
– Type 4: Isolated hilar stricture
May mimic cholangiocarcinoma
• Size
Variable: Focal or diffuse involvement of biliary tree
• Morphology
Concentric bile duct wall thickening and hyperenhancement
Typically long smooth stricture with upstream biliary ductal dilatation
Radiographic Findings
• ERCP
Distal CBD stricture and irregularity of main pancreatic duct (due to concomitant AIP) most frequent findings
Strictures of intra- and extrahepatic ducts rarely occur without pancreatic duct involvement
Long, smooth strictures (particularly of distal CBD) without irregularity
CT Findings
• Circumferential focal or diffuse bile duct wall thickening
Most commonly affects distal CBD, but can affect any portion of biliary tree
Hyperenhancement of affected bile duct: Enhancement may persist during delayed phase
No vascular invasion, metastatic disease, or other secondary findings of malignancy
• No clear association between ISC and malignancy, but involved sites in biliary tree may rarely appear mass-like and mimic malignancy (inflammatory pseudotumor)
• Diffuse gallbladder wall thickening (due to either lymphoplasmacytic infiltration and transmural fibrosis or superimposed cholecystitis)
• Findings of concomitant autoimmune pancreatitis
Focal, multifocal, or diffuse (sausage-shaped) pancreatic enlargement with hypodense pancreatic capsule
Enlargement of pancreas with a paucity of peripancreatic inflammation, fluid, or stranding
Less enhancement than expected in arterial phase; parenchyma/capsule may show delayed enhancement
Only gold members can continue reading. Log In or Register to continue



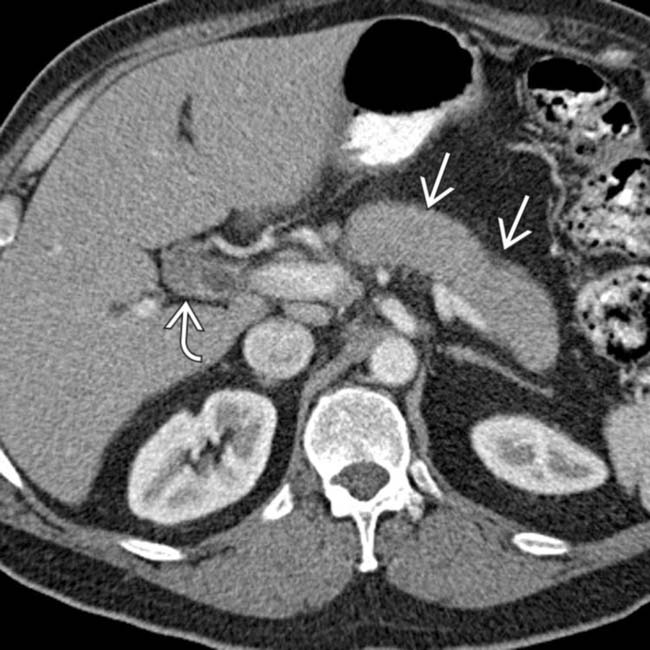
 and an enlarged, sausage-shaped pancreas
and an enlarged, sausage-shaped pancreas  . The appearance of the pancreas is consistent with autoimmune pancreatitis (AIP), and an elevated IgG4 indicates that the bile duct thickening is due to IgG4-related sclerosing cholangitis (ISC).
. The appearance of the pancreas is consistent with autoimmune pancreatitis (AIP), and an elevated IgG4 indicates that the bile duct thickening is due to IgG4-related sclerosing cholangitis (ISC).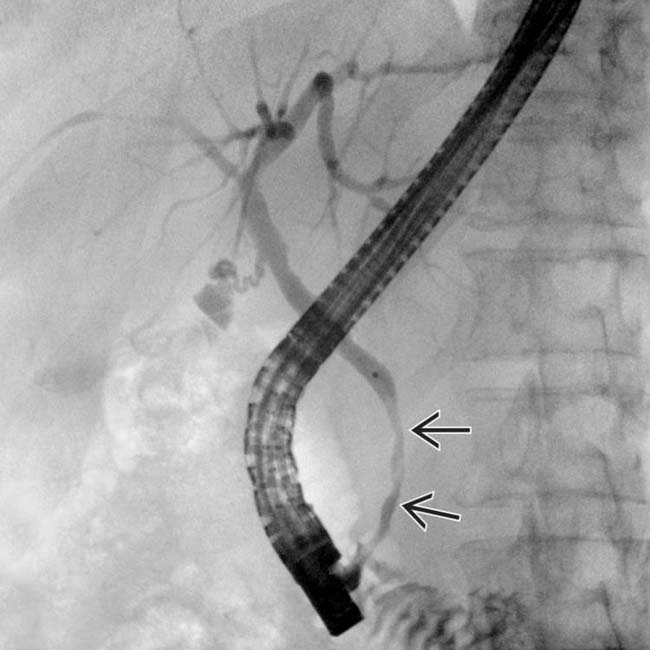
 of the distal CBD, the most common manifestation of ISC. ISC and AIP resolved after steroid and azathioprine therapy.
of the distal CBD, the most common manifestation of ISC. ISC and AIP resolved after steroid and azathioprine therapy.
 with wall hyperenhancement, compatible with autoimmune cholangitis.
with wall hyperenhancement, compatible with autoimmune cholangitis.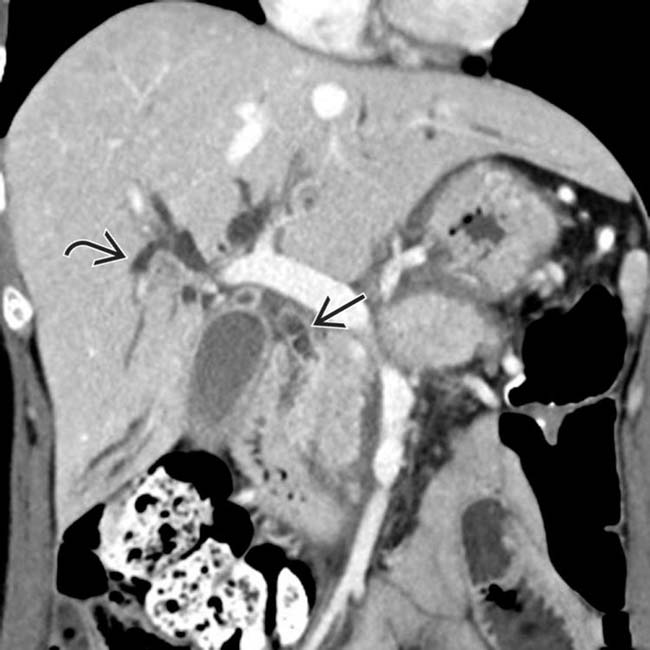
 with proximal biliary dilatation
with proximal biliary dilatation  , in keeping with IgG4-related cholangitis.
, in keeping with IgG4-related cholangitis.
















 Focal, multifocal, or diffuse (sausage-shaped) pancreatic enlargement with hypodense pancreatic capsule
Focal, multifocal, or diffuse (sausage-shaped) pancreatic enlargement with hypodense pancreatic capsule






