Massively dilated bile ducts (either diffuse or localized) filled with mucin
Mural nodules best visualized after removal of mucin
Biliary dilation both proximal and distal to mural nodule
• CT/MR: Markedly dilated intra-/extrahepatic bile ducts with mural nodularity or discrete intraductal mass
Attenuation and MR signal characteristics of mucin distending ducts is similar to normal bile
Presence of mural nodularity or soft tissue suggests presence of malignancy
PATHOLOGY
• Unknown etiology, but associations with hepatolithiasis and Clonorchis suggest chronic biliary inflammation may be causative
CLINICAL ISSUES
• Most common in elderly patients from East Asia
• May present with repeated episodes of cholangitis and jaundice
• Biliary IPMN localized to intrahepatic ducts may be treated with partial hepatectomy if tumor is relatively localized
• Resection of the common duct with Roux-en-Y anastomosis may be required for tumors involving either extrahepatic duct or right/left main ducts
• Stenting or drainage to alleviate jaundice in patients who are not surgical candidates
• Multifocality frequent, and recurrences after surgery are common due to small foci of undetected disease in biliary tree distant from site of resection
(Left) Graphic of biliary intrapapillary mucinous tumor demonstrates the segmental distension of the right lobe intrahepatic ducts , which are filled with mucin and contain a mucosal mass arising from the ductal epithelium.
(Right) Axial T1WI MR with gadolinium in a woman with midepigastric pain and elevated alkaline phosphatase shows fusiform dilatation of the left bile ducts , which proved to be biliary IPMN at surgery.
(Left) Axial CECT in a patient presenting with RUQ pain and elevated alkaline phosphatase demonstrates atrophy of the left lobe and marked dilation of the left bile duct greater than the right. ERCP and subsequent surgery revealed a left duct biliary IPMN.
(Right) Axial CECT shows asymmetric left biliary ductal dilatation and subtle enhancing nodularity within the proximal left duct . Intraductal cholangiocarcinoma and background biliary IPMN were identified at histology. (Courtesy S. Yeon Kim, MD.)
TERMINOLOGY
Abbreviations
• Intraductal papillary mucinous neoplasm (IPMN) of bile ducts
Synonyms
• Intraductal papillary neoplasm of liver, mucin-secreting biliary papillomatosis, mucin-producing cholangiocarcinoma, mucinous ductal ectasia of biliary tree
Definitions
• Mucin-producing papillary neoplasm arising from biliary mucosa
Only recently added to WHO classification in 2010
Significant overlap with biliary papillomatosis, and some authors suggest they are same entity
IMAGING
General Features
• Best diagnostic clue
Diffuse segmental “aneurysmal” dilation of bile ducts with a polypoid or nodular intraductal mass
Biliary dilation both proximal and distal to mural nodule due to mucin hypersecretion
• Location
Intra-/extrahepatic bile ducts: Most common locations are left liver lobe ducts and liver hilum
• Size
• Morphology
“Aneurysmal,” marked dilatation of mucin-distended ducts
Radiographic Findings
• ERCP
Extrusion of clear mucin from patulous ampulla visible to endoscopist due to mucin hypersecretion by tumor
Massively dilated bile ducts (either diffuse or localized) filled with mucin
– Mucin-filled bile ducts may result in nonvisualization of affected segment(s) due to difficulty of filling mucin-filled ducts with contrast
– Amorphous filling defects in dilated ducts may representing either mucin plugs or tumor
Mural nodules best visualized after removal of mucin
CT Findings
• Markedly dilated intra-/extrahepatic bile ducts with mural nodularity or discrete intraluminal papillary/fungating mass
Attenuation of mucin distending ducts is similar to normal bile
– Mucin within ducts cannot be differentiated from normal bile on CT
Presence of mural nodularity or soft tissue component should suggest presence of malignancy
• CT cholangiography may play a role in preoperative diagnosis and determination of tumor resectability: Mucin (and tumor) outlined by biliary contrast
MR Findings
• Diffuse or segmental biliary ductal dilatation with bile duct contents appearing hyperintense on T2WI and hypointense on T1WI (similar to normal bile)
Mucin within ducts cannot be differentiated from normal bile on MR
ERCP/MRCP mismatch: Mucin-filled duct is not visible on ERCP while it is seen on MRCP
Hepatobiliary contrast agents (i.e., Eovist) may demonstrate nonfilling of affected ducts (i.e., those filled with mucin), similar to ERCP
• Papillary projections or discrete soft tissue masses within dilated ducts appear hypointense on T1WI, hyperintense on T2WI, and enhancing on T1WI C+
Enhancing mural nodularity raises concern for malignancy
Ultrasonographic Findings
• Grayscale ultrasound
Complex “mass” of aneurysmally dilated bile ducts
Echogenic intraductal masses juxtaposed against anechoic mucin filling duct
Linear echoes within dilated ducts may suggest mucobilia (layer sign)
No flow in dilated bile ducts
Only gold members can continue reading. Log In or Register to continue





 , which are filled with mucin and contain a mucosal mass
, which are filled with mucin and contain a mucosal mass  arising from the ductal epithelium.
arising from the ductal epithelium.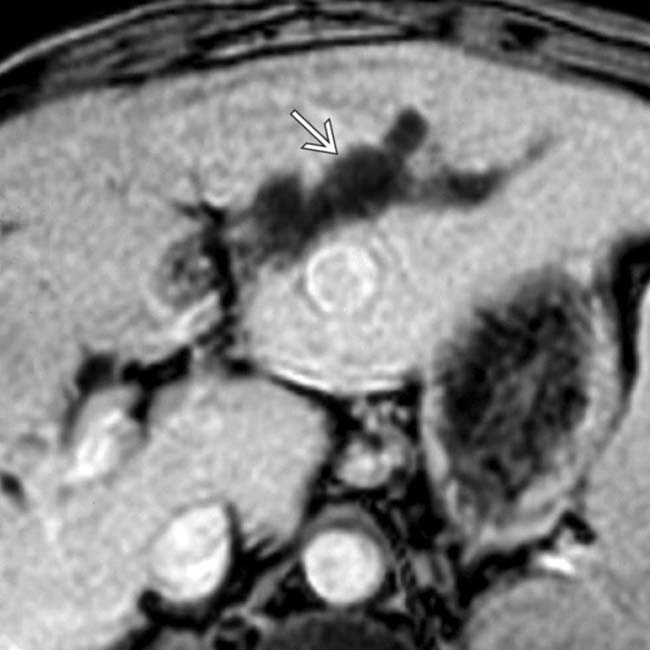
 , which proved to be biliary IPMN at surgery.
, which proved to be biliary IPMN at surgery.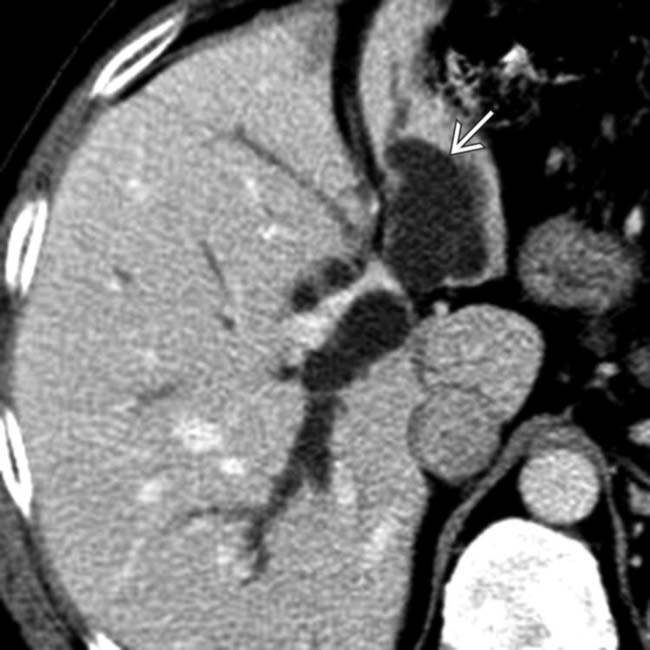
 greater than the right. ERCP and subsequent surgery revealed a left duct biliary IPMN.
greater than the right. ERCP and subsequent surgery revealed a left duct biliary IPMN.
 and subtle enhancing nodularity within the proximal left duct
and subtle enhancing nodularity within the proximal left duct  . Intraductal cholangiocarcinoma and background biliary IPMN were identified at histology. (Courtesy S. Yeon Kim, MD.)
. Intraductal cholangiocarcinoma and background biliary IPMN were identified at histology. (Courtesy S. Yeon Kim, MD.)






 Extrusion of clear mucin from patulous ampulla visible to endoscopist due to mucin hypersecretion by tumor
Extrusion of clear mucin from patulous ampulla visible to endoscopist due to mucin hypersecretion by tumor Massively dilated bile ducts (either diffuse or localized) filled with mucin
Massively dilated bile ducts (either diffuse or localized) filled with mucin















