Chapter 16 Biological and pathological introduction
Neoplasia
Benign and malignant neoplasms
Neoplasia is not a single disease, but rather a common pathological process with a multitude of different varieties and clinical outcomes. One fundamental division is between benign and malignant tumours. Benign tumours will remain localized, with generally relatively little effect on the patient. In contrast, other tumours are locally destructive, may spread to involve other parts of the body, and ultimately result in the death of the patient. Figure 16.1 and Table 16.1 show some of the differences between benign and malignant neoplasms. Further aspects of the classification of tumours are discussed later in this chapter.
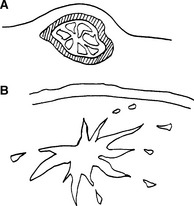
Table 16.1 Characteristics of neoplasms
| Feature | Benign | Malignant |
|---|---|---|
| Growth rate | Slow | Variable, may be rapid |
| Margin | Encapsulated | Invasive |
| Local effect | Little | Destructive |
| Differentiation | Good | Variable, may be poor |
| Metastases | No | Frequently |
| Usual outcome | Good | Fatal |






