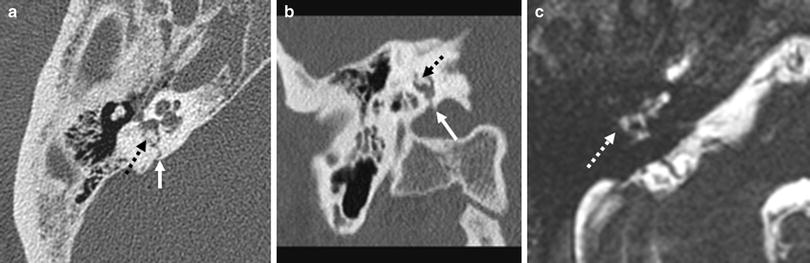
Fig. 1
Longitudinal fracture of the anterior subtype. Fall on the head, after 3 days an incomplete peripheral facial nerve palsy has developed. Fracture lines through the anterior squamous portion of the temporal bone (white arrows) and opacifications (stars) in the mastoid and tympanic cavity especially at the fossa geniculi as expression of bleedings. a, b CT axial; c, d CT coronal
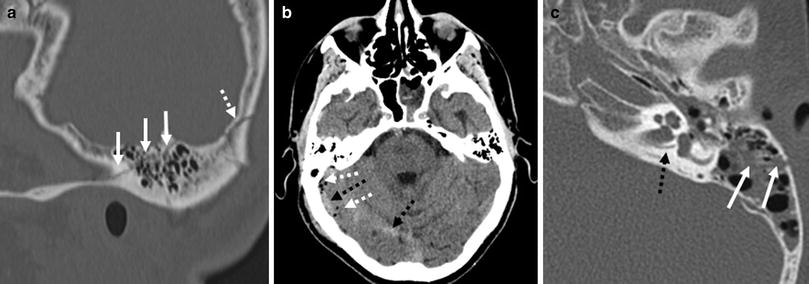
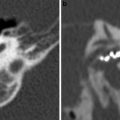
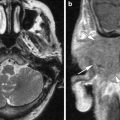
Fig. 2
Longitudinal fractures of the posterior subtype. Fall in alcoholised condition (a, b). A cupboard fell on the head (c). Fracture lines through the mastoid (white arrows in a and c) and occipital bone (dotted arrow in a), intracranial air (white dotted arrows in b) and infratentorial subdural haematoma (black dotted arrows in b). The prominent singular canal (black dotted arrow in c) should not be confused with a fracture. a CT sagittal; b brain CT axial; c CT axial
Compared to transverse fractures facial nerve palsy occurs more seldom (10–20 %). Mostly, it is delayed, incomplete and transitory, caused by pressure of an extraneural haematoma on the nerve. Dural lacerations with a CSF leak may occur, but most leaks close spontaneously. As late complication the development of a cholesteatoma is observed. (Gladwell and Viozzi 2008; Jäger et al. 1997; Kösling and Neumann 2010; Rafferty et al. 2006; Schuknecht and Graetz 2005; Turetschek et al. 1997).
Clinical findings:
Palpable step in the external auditory canal
Perforation of the drum
Haemtotympanum
Conductive hearing loss
Otoliquorrhea; in intact drum ‘false rhinoliquorrhea’ (drainage via the tuba auditiva)
Peripheral facial nerve palsy.
Radiological findings:
Anterior subtype (more common): fracture line(s) through the anterior and/or middle squamous portion of the temporal bone, the anterior wall of the external auditory canal, the tegmen tympani, toward the geniculate ganglion and possibly along the anterior border of the petrous portion or through the tuba auditiva (Fig. 1), rarely extend into the central skull base
Posterior subtype (less common): fracture line(s) through the posterior squamous portion of the temporal bone or through the mastoid process, the posterior wall of the external auditory canal, the second knee of the facial nerve or its mastoid portion and may extend to the surrounding of the foramen lacerum and seldom into the jugular foramen (Fig. 2)
Attendant signs in both subtypes: opacifications of the mastoid, cavum tympani and external auditory canal—sometimes with fluid levels as expression of bleedings (Figs. 1, 2); injuries of ossicles (see below); occasionally involvement of the carotid canal; rarely intracranial air as a sign for an open skull base fracture (Fig. 2b).
Differential diagnosis:
Small canals, fine sutures (pseudofractures) (Fig. 2c)—comparison with the contralateral side (when it is unaffected) helps in the differentiation.
Important points:
Knowledge of the clinical findings supports the radiological assessment
Analyze the roof of the middle ear and mastoid carefully on coronal reconstructions; traumatic gaps may occur with CSF leaks and can lead to cephaloceles and/or meningitis (Fig. 3)
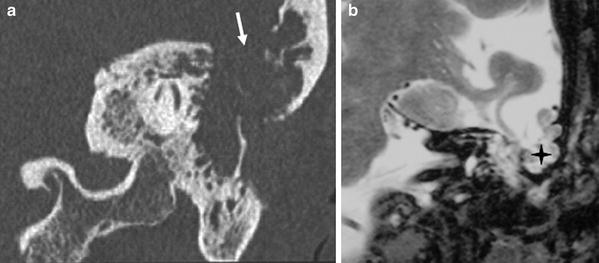
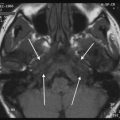
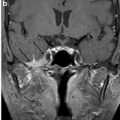
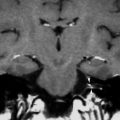
Fig. 3
Post-traumatic meningoencephalocele. Head trauma many years ago. On CT a broad gap in the roof of the mastoid is visible (arrow in a). MRI demonstrates the prolapse of brain into the mastoid (star). a CT coronal; b MRI T2-w coronal. (b with permission from Kösling and Neumann (2010))
The canal of the ICA and facial nerve has to be analysed carefully, but not each fracture line is linked with an injury of the vessel and nerve, respectively
Dislocated fragments of the carotid canal should implicate a non-invasive imaging of cerebral arteries or DSA (depending on the available technique, no unique recommendations)
Fracture lines through the jugular foramen are extremely rarely accompanied by venous complications (Saraiya and Aygun 2009).
2.2 Transversal Fractures
Transversal fractures arise from frontal or occipital directed forces. They are less common (about 20 % of all temporal bone fractures). Fractures pass off perpendicular to the long axis of the petrous bone and can be linked with a damage of the inner ear (Figs. 4, 5). Transversal fractures can be further differentiated into a lateral and medial subtype.
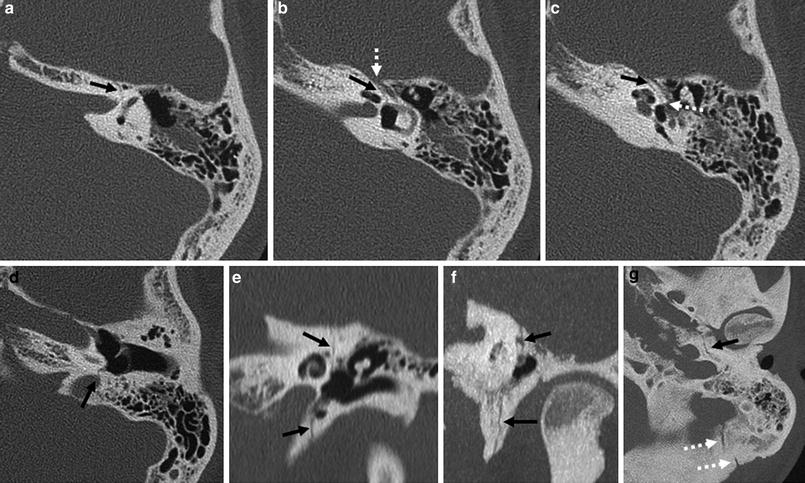
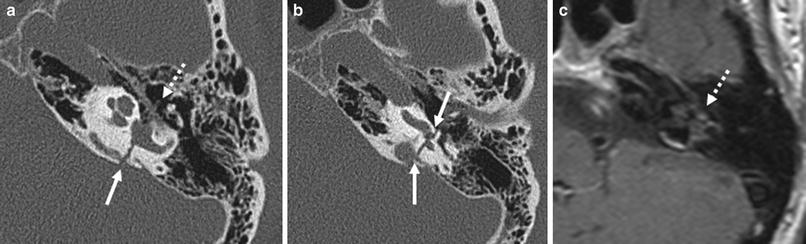
Fig. 4
Transversal fracture of the lateral subtype. Traumatic brain injury of first degree. Fracture lines (black arrows) through the otic capsule with involvement of the labyrinth, the fossa geniculi (white dotted arrow in b), the oval window (white dotted arrow in c), the jugular fossa (arrow in d) as well as a described opacification in the antrum. The occipitomastoid suture (white dotted arrows in g) should not be confused with a fracture. a–d CT axial; e CT coronal; f CT coronal thin-sliced maximum intensity projection; g CT axial thin-sliced maximum intensity projection
Fig. 5
Transversal fracture of the lateral subtype. Motor vehicle accident, immediate peripheral facial nerve palsy. On CT fracture lines (white arrows) through the labyrinth including the jugular foramen and subtle opacifications around the tympanic segment of the facial nerve (dotted white arrow in a). On MRI an enhancement of the tympanic segment of the facial nerve is visible (dotted white arrow in c). a, b CT axial; c MRI T1-w with contrast medium, axial. (a, c with permission from Kösling and Neumann (2010))
A mostly immediate and complete facial nerve palsy, which is caused by a direct damage of the nerve, is found in about half of cases. From the lateral subtype, labyrinthine fistulas may result. Fibrosing and ossification of the labyrinth are possible serious sequelae (Fig. 6) (Gladwell and Viozzi 2008; Jäger et al. 1997; Kösling and Neumann 2010; Rafferty et al. 2006; Schuknecht and Graetz 2005; Turetschek et al. 1997).