Fig. 21.1
MRI findings (fat suppression, fluid sensitive sequence) of bone marrow edema syndrome showing marked, bright, hyperintense signal in left femoral head and neck
Fig. 21.2
MRI findings (T1 sequence) of bone marrow edema syndrome showing dark, hypointense signal in left femoral head and neck
In ON, edema at the hyperintense T2 band on the edge of necrosis may also potentially cause pain as opposed to the diffuse, regional marrow edema seen in BMES. However, in ON, this pain may or may not correlate with the stage or extent of anatomic involvement of the bone [1]. Patients with these symptoms typically have diffuse, polyostotic ON involving both subchondral and large metaphyseal infarcts and present with diffuse bone pain, analogous to sickle cell disease patients. Commonly, this will occur in ON related to steroid usage for either bone marrow transplantation or treatment of acute lymphoblastic leukemia (Fig. 21.3).

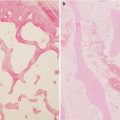
Fig. 21.3
A case example of polyostotic ON involving bilateral distal femur and proximal tibia (a, b), femoral head and proximal femora (c), and proximal humerus (d, e) as seen on MR
21.3.2 Subchondral Fractures
These are the fractures through the necrotic subchondral bone which most often occurs in the superolateral aspect of the femoral head [8]. This classical finding is seen as a “crescent sign” on radiographs in ARCO stage 3 disease and is responsible for increasing pain with activity in stage 3 of the disease process. These fractures may also lead to instability of the overlying articular cartilage with loss of fixation to the subchondral bone occurring (Fig. 21.4a, b). At times a gap may develop between the subchondral bone and overlying cartilage leading to a joint effusion (Fig. 21.5).
Fig. 21.4
(a, b) A case example of underlying detachment of the cartilage from the bone in the femoral head seen during hip replacement surgery
Fig. 21.5
MRI STIR sequence with contrast showing ON with subchondral fracture in the pre-collapse stage. Note the unilateral synovial effusion in the left symptomatic hip and absence of effusion in the right asymptomatic hip
21.3.3 Degenerative Joint Disease
The unstable articular cartilage eventually will fracture at the margin of the subchondral bone depression resulting in a loose flap of cartilage. This is associated with flattening of the femoral head and the loss of contour initiates the early degenerative cascade with subsequent advanced degenerative changes responsible for pain either at rest or with minimal activity [2]. The etiology of persistent disabling pain in late stages of ON involves degenerative joint disease that is a combination of joint effusion, synovitis, osteochondral fragments, and a bone-on-bone erosive process that is similar to the end-stage osteoarthritis from any other cause.
21.4 Causes of Pain in Different Stages of Disease
As there are multiple causes for pain in ON, they may vary depending upon the specific stage of disease (ARCO staging Table 21.1) [9].
Table 21.1
Schematic modified outline of the five-stage Association Research Circulation Osseous (ARCO) international classification for osteonecrosis of the femoral head (Reproduced with permissions ARCO [9])
21.4.1 ARCO Stage 1
By definition, there is no subchondral fracture. Most of the patients are asymptomatic. If a patient has pain, it is likely due to the onset of intraosseous hypertension because of abnormally high content of fluid in the bone marrow secondary to acute bone marrow ischemia. In this stage mild pain can also be perceived as severe by some patients [5].
21.4.2 ARCO Stage 2
Localized osteopenia, marrow necrosis, and bone infarcts are possibly responsible for the dull aching pain in this stage [2]. Patients that have polyostotic disease with large metaphyseal infarcts typically have diffuse poorly localized, vague, non-activity-related pain. This likely is due to elevated intraosseous pressure and/or marrow edema accentuated by the large infarcts. In some patients, a synovial effusion is present despite the absence of a demonstrable subchondral fracture (Fig. 21.3). As is typical for any synovial effusion, the distended joint capsule is symptomatic. Some patients with ARCO stage 2 ONFH may be asymptomatic as well. During this stage, in the absence of a synovial effusion, determining whether or not a patient’s pain is due to ON or some other etiology can be challenging (Fig. 21.6a–c).
Fig. 21.6
ARCO stage 2 bilateral disease of femoral head that with bilateral small effusions on MR but symptomatic on only one side
21.4.3 ARCO Stage 3
21.4.4 ARCO Stage 4
The irregularity of the articular surface initiates fissures in the cartilage, subsequently followed by onset of advanced degenerative joint disease with corresponding changes on both sides of a joint (e.g., acetabulum) and worsening pain both at rest and with activity [2].
21.5 Clinical Features and Presentation
The most accurate clinic-radiological data comes from prospective screening studies performed in high-risk patient groups [1, 11–14].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


